Edition: Metabolic Disease
14 March, 2026
In The News
Vol 1, Edition 9
What Is Metabolic Syndrome — The Silent Condition Affecting 1 in 3 Americans
Most people who have metabolic syndrome don’t know it. There’s no single or dramatic symptom — just a cluster of five measurable risk factors that, together, signal a metabolism in serious trouble. Understanding what metabolic syndrome is, how to recognize it, and what drives it is the first step toward reversing it.

Published By: MAP30 Challenge
Authored By: John Shaw
A common assumption is that metabolic disease announces itself — that you’ll feel sick, get a diagnosis, and then take action. Metabolic syndrome doesn’t work that way. It develops silently over years, often with no symptoms at all, while quietly elevating the risk of type 2 diabetes, cardiovascular disease, stroke, and early mortality. By the time most people learn they have it, the underlying hormonal dysfunction has been building for a decade.
Metabolic Syndrome Definition and the 5 Diagnostic Criteria
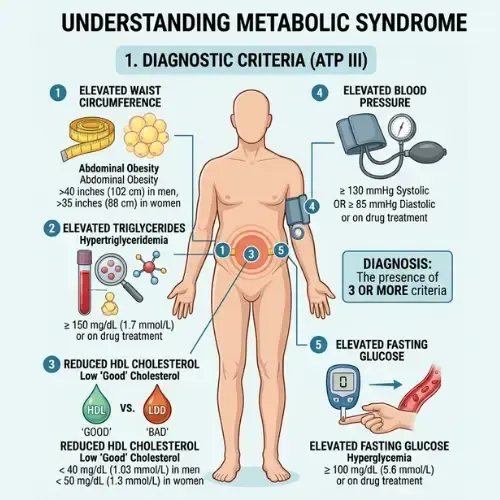
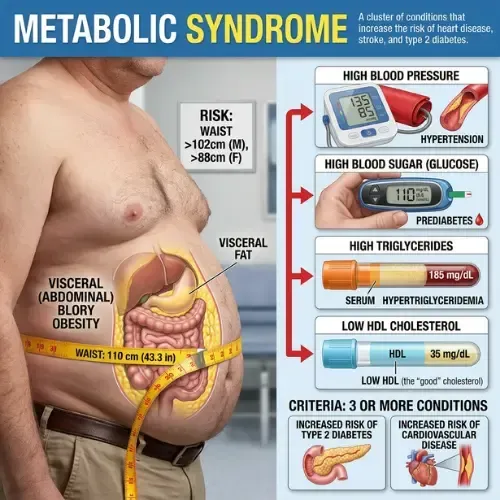
Metabolic syndrome is not a single disease. It is a cluster of five interconnected metabolic abnormalities that, when present together, dramatically increase the risk of type 2 diabetes, heart disease, stroke, and non-alcoholic fatty liver disease. According to the National Cholesterol Education Program Adult Treatment Panel III — the most widely used clinical definition — a diagnosis of metabolic syndrome requires three or more of the five criteria.
The five criteria are:
1. elevated waist circumference
2. Elevated triglycerides
3. Low HDL cholesterol
4. Elevated blood pressure
5. Elevated fasting blood glucose
Each of these markers, in isolation, represents a manageable risk factor. Together, they represent a systemic breakdown in the body’s ability to regulate insulin, glucose, and fat metabolism — a condition with a single upstream driver.
That driver is insulin resistance. Every one of the five criteria is either caused by, worsened by, or directly connected to chronically elevated insulin and the cellular dysfunction that follows. Metabolic syndrome, understood correctly, is insulin resistance made visible across five separate clinical measurements.
“Metabolic syndrome is not five separate problems. It is one problem — insulin resistance — showing up in five different measurements at the same time.”
How Common Is Metabolic Syndrome — And Who Is Most at Risk
The table below shows the five clinical thresholds used to diagnose metabolic syndrome, along with the metabolic mechanism behind each one. Three or more of these criteria present simultaneously constitutes a diagnosis.
> 35" women Visceral fat surrounding internal organs — the primary metabolic driver of the cluster
< 50 mg/dL women Suppressed by the same metabolic environment that elevates triglycerides
Meeting three of these five criteria is the clinical threshold. But the research is unambiguous: even two criteria present simultaneously signals significant metabolic dysfunction and elevated long-term risk. Waiting for a formal diagnosis before taking action means waiting until the condition is already well established.
How Common Is Metabolic Syndrome — And Who Is Most at Risk
The American Heart Association and the National Heart, Lung, and Blood Institute estimate that approximately one in three American adults meets the criteria for metabolic syndrome. That figure — roughly 35% of the adult population — has increased steadily over the past four decades, tracking almost exactly with the rise of processed food consumption and sedentary behavior.
Age is a significant risk factor. Prevalence rises sharply after age 40 and exceeds 50% in adults over 60. But metabolic syndrome is no longer confined to older populations. Rates among adults aged 20 to 39 have increased substantially, driven by the same dietary patterns that affect older cohorts: high refined carbohydrate intake, excess added sugar, and low dietary fiber.
Ethnicity also plays a role. Hispanic Americans show the highest prevalence rates, followed by non-Hispanic whites, with African Americans and Asian Americans showing distinct risk profiles based on body composition and genetic insulin sensitivity factors. However, the dietary and lifestyle drivers are consistent across all populations.
🧠
U0001f52c CLINICAL STUDY — Aguilar M et al. (2015)
"Prevalence of the Metabolic Syndrome in the United States, 2003–2012." JAMA, 313(19), 1973–1974.
Analysis of NHANES data from 2003 to 2012 found that metabolic syndrome prevalence among US adults was 34.7% overall — with rates rising with age and varying significantly by sex and ethnicity. The study confirmed that metabolic syndrome prevalence had not declined despite decades of public health messaging around diet and exercise.
What This Means: One in three Americans already meets the clinical criteria. The majority are unaware. Routine screening for all five markers — not just fasting glucose and blood pressure — is essential for early identification.
Why Metabolic Syndrome Is Called the Silent Condition
The reason metabolic syndrome goes undiagnosed for years — sometimes decades — is that it produces no single obvious symptom. Each of the five criteria can be present at subclinical levels for years before any individual marker crosses the diagnostic threshold. And most standard medical appointments do not test for all five simultaneously.
A typical annual physical might measure blood pressure and fasting glucose. It is unlikely to include a fasting triglyceride panel, an HDL measurement, and a waist circumference assessment in the same appointment. Yet it is only when all five are assessed together that the pattern becomes visible.
The result is a large population carrying significant metabolic risk who have been told their individual numbers are “a little high” or “borderline” — without anyone connecting those borderline numbers into a clinical picture that has a name, a mechanism, and a proven intervention pathway.
Why This Matters: The Upstream Problem
Type 2 diabetes does not emerge suddenly. It develops at the end of a progression that typically begins with insulin resistance, advances through metabolic syndrome, and eventually crosses the diagnostic threshold for prediabetes and then type 2 diabetes. Metabolic syndrome is the stage in that progression where intervention is most effective — and most often missed. Identifying and addressing it at this stage can prevent type 2 diabetes entirely.
What Causes Metabolic Syndrome? Insulin Resistance
Understanding metabolic syndrome requires understanding why five apparently separate measurements are actually one condition. The connection is insulin — specifically, what happens when cells stop responding to it normally.
When muscle, liver, and fat cells become resistant to insulin’s signal, the pancreas compensates by producing more insulin to achieve the same effect. This chronically elevated insulin state — hyperinsulinemia — is the central driver of every criterion in the metabolic syndrome cluster.
How hyperinsulinemia produces each criterion:
Waist circumference: Elevated insulin promotes visceral fat storage via glucocorticoid receptor activation in abdominal adipose tissue. Visceral fat is metabolically active and itself worsens insulin resistance — a self-reinforcing cycle.
Triglycerides: The liver converts excess glucose — which cannot enter insulin-resistant muscle cells — into triglycerides via de novo lipogenesis. Chronically elevated insulin drives this process continuously.
HDL cholesterol: High triglyceride production displaces HDL particles. The same metabolic environment that raises triglycerides suppresses HDL synthesis and accelerates HDL clearance.
Blood pressure: Insulin resistance impairs the kidneys’ ability to excrete sodium, leading to fluid retention and elevated vascular pressure. Insulin also stimulates the sympathetic nervous system, raising heart rate and arterial tension.
Fasting blood glucose: As insulin resistance progresses, the liver releases glucose overnight via gluconeogenesis even when blood glucose is already adequate. Elevated fasting glucose is the liver overriding insulin’s suppression signal.
Address insulin resistance and all five markers improve. That is not a coincidence — it is the mechanistic proof that metabolic syndrome is one condition with one upstream driver.
The Best Diet for Metabolic Syndrome — What the Evidence Actually Shows
The most direct dietary intervention for metabolic syndrome is the one that addresses its root cause: reducing the chronic insulin demand that drives insulin resistance. That means reducing refined carbohydrates and added sugars — the dietary components that produce the largest and most sustained insulin responses.
A 2020 meta-analysis published in PLOS Medicine, reviewing 61 randomized controlled trials involving over 6,500 participants, found that low-carbohydrate diets produced significantly greater reductions in triglycerides, blood pressure, fasting glucose, and waist circumference than low-fat diets at equivalent calorie levels. These are four of the five metabolic syndrome criteria improving simultaneously from a single dietary intervention.
The practical application is straightforward: eliminate added sugars and high-fructose corn syrup, reduce refined grains (bread, pasta, white rice, processed cereals), prioritize protein and dietary fat as the primary caloric sources, and increase non-starchy vegetables for fiber and micronutrient density. This dietary pattern consistently reduces fasting insulin, which is the upstream variable all five criteria depend on.
U0001f52c CLINICAL STUDY — Meng Y et al. (2017)
"Efficacy of low carbohydrate diet for type 2 diabetes mellitus management: A systematic review and meta-analysis of randomized controlled trials." Diabetes Research and Clinical Practice, 131, 124–131.
Meta-analysis of randomized controlled trials found that low-carbohydrate dietary interventions produced significant improvements in fasting glucose, HbA1c, triglycerides, and HDL cholesterol compared to control diets — addressing four of the five metabolic syndrome criteria simultaneously. Effects were most pronounced in the first three to six months and remained clinically meaningful at twelve months.
What This Means:
Dietary carbohydrate reduction is not a peripheral intervention for metabolic syndrome. It targets the central mechanism — insulin demand — and produces measurable improvements across the full diagnostic cluster.
Metabolic Syndrome Treatment — Beyond Diet
Diet is the primary lever, but metabolic syndrome treatment is most effective when it addresses the full hormonal environment. Four additional interventions have strong clinical support:
Resistance and aerobic exercise
Skeletal muscle is the largest site of glucose disposal in the body. Exercise — both resistance training and aerobic — acutely improves insulin sensitivity independent of weight loss by increasing GLUT4 transporter expression in muscle cells. Regular exercise is the only intervention that directly improves the muscle-side component of insulin resistance.
Sleep quality and duration
Even a single night of poor sleep measurably increases insulin resistance by the following morning. Chronic sleep deprivation is an independent driver of all five metabolic syndrome criteria. Seven to nine hours of consistent, quality sleep is not optional for metabolic recovery — it is a primary intervention.
Visceral fat reduction
Visceral fat is not metabolically inert. It actively secretes inflammatory cytokines — including TNF-alpha and IL-6 — that worsen insulin resistance systemically. Reducing visceral fat, which responds preferentially to carbohydrate restriction, produces improvements in all five metabolic syndrome markers simultaneously because it reduces the inflammatory load driving the condition.
Stress and cortisol management
Chronically elevated cortisol directly promotes visceral fat storage and suppresses insulin sensitivity. For people with metabolic syndrome who also carry significant psychological or physiological stress, cortisol management — sleep, moderate exercise, and deliberate parasympathetic activation — is a meaningful metabolic intervention, not a lifestyle extra.
GLP-1 Medications
For people with severe metabolic syndrome who have not responded to lifestyle intervention, GLP-1 receptor agonists like semaglutide (Ozempic) produce measurable improvements across multiple metabolic syndrome criteria simultaneously. However, the research is clear that these improvements are contingent on continued drug use — when GLP-1 drugs are stopped, metabolic markers return toward baseline. The full picture of what these drugs do, what they don't do, and how to support GLP-1 naturally is covered in the Ozempic and GLP-1 article in this library.
The Bottom Line on Metabolic Syndrome Treatment
There is no single medication that addresses all five metabolic syndrome criteria simultaneously. There is one dietary intervention that does: reducing chronic insulin demand through carbohydrate restriction. Combined with resistance exercise, quality sleep, and visceral fat reduction, this approach addresses the root cause rather than managing individual markers in isolation. That is the difference between treating a diagnosis and reversing a condition.
Metabolic Syndrome and Longevity — What the Long-Term Data Shows
The long-term consequences of untreated metabolic syndrome extend well beyond type 2 diabetes. A 2004 meta-analysis published in Diabetes Care, reviewing data from 37 studies involving over 170,000 participants, found that individuals with metabolic syndrome had a twofold increase in cardiovascular disease risk and a fivefold increase in type 2 diabetes risk compared to those without the condition.
More recent longevity research has established metabolic syndrome as one of the most reliable predictors of all-cause mortality in middle-aged adults — more predictive than any single cardiovascular risk factor in isolation. The cluster effect is the key: it is not elevated triglycerides alone, or elevated blood pressure alone, but the simultaneous presence of multiple markers of the same underlying dysfunction that drives the risk.
The corollary is equally important: the research on reversal is consistent. Addressing the root cause — insulin resistance — through dietary carbohydrate reduction, exercise, and sleep produces measurable improvements in all five criteria within weeks to months, and those improvements translate directly to reduced cardiovascular and diabetes risk. Metabolic syndrome is not a permanent diagnosis. It is a reversible metabolic state.
“Metabolic syndrome is one of the most reliable predictors of early mortality in middle-aged adults — and one of the most responsive conditions to targeted dietary intervention. The biology works both ways.”
What This Means for the MAP30 Challenge
The MAP30 Challenge is designed around the metabolic principles that reverse metabolic syndrome at the root. The dietary framework reduces the chronic insulin demand that drives all five criteria. The movement protocols are calibrated to improve insulin sensitivity directly. The sleep framework addresses one of the most commonly overlooked metabolic variables.
If you have been told your numbers are “a little high” in more than one area — blood pressure, fasting glucose, triglycerides, waist circumference — that pattern has a name, a mechanism, and a proven intervention pathway. MAP30 addresses all of it simultaneously, because all of it has the same upstream cause.
This article is part of our Metabolic Disease series. Metabolic Disease
Latest Articles

Insulin Resistance
You don't need a diabetes diagnosis to have insulin resistance. Millions of Americans are living with it right now — tired, foggy...

Calorie Deficit Diet?
The calorie deficit model has been the foundation of weight loss advice for over a century. But millions of people follow it precisely...

The Food Pyramid
For three decades, Americans were told to eat 6 to 11 servings of grains per day and avoid fat at all costs. The science behind that advice was always...

John Shaw
MAP30 Challenge
John Shaw is a Certified Nutrition Educator and the founder of the MAP30 Challenge. What began as a personal health journey at 294 pounds, and pre-diabetic, evolved into a structured 30-day metabolic reset program grounded in nutritional science. John's mission is simple: give people the biological education that the diet industry never did.
Disclaimer: The information in this article is for educational and historical context only and does not constitute medical or dietary advice. Nutritional science is an evolving field and individual dietary needs vary. Consult a qualified healthcare provider or registered dietitian before making significant changes to your diet or health management plan.
FAQ's
1. What is metabolic syndrome?
Metabolic syndrome is a cluster of five interconnected metabolic abnormalities that together significantly increase the risk of type 2 diabetes, heart disease, and stroke. The five criteria are: elevated waist circumference, elevated triglycerides, low HDL cholesterol, elevated blood pressure, and elevated fasting blood glucose. A diagnosis requires three or more of these five markers to be present simultaneously. The underlying driver of all five is insulin resistance.
2. What are the 5 criteria for metabolic syndrome?
The five diagnostic criteria are: (1) Waist circumference above 40 inches in men or 35 inches in women; (2) Triglycerides at or above 150 mg/dL; (3) HDL cholesterol below 40 mg/dL in men or below 50 mg/dL in women; (4) Blood pressure at or above 130/85 mmHg; (5) Fasting blood glucose at or above 100 mg/dL. Three or more of these criteria present simultaneously constitutes a clinical diagnosis of metabolic syndrome.
3. What causes metabolic syndrome?
The primary driver of metabolic syndrome is insulin resistance — a condition in which muscle, liver, and fat cells stop responding normally to insulin. Chronically elevated insulin (hyperinsulinemia), caused by sustained high carbohydrate and sugar intake, drives all five diagnostic criteria simultaneously. Secondary contributors include physical inactivity, poor sleep, chronic stress and elevated cortisol, visceral fat accumulation, and genetic susceptibility.
4. What is the best diet for metabolic syndrome?
The most evidence-supported dietary intervention for metabolic syndrome is carbohydrate restriction — specifically eliminating added sugars, high-fructose corn syrup, and refined grains. A 2020 PLOS Medicine meta-analysis of 61 randomized controlled trials found low-carbohydrate diets produced significantly greater improvements in triglycerides, blood pressure, fasting glucose, and waist circumference than low-fat diets. These are four of the five metabolic syndrome criteria improving simultaneously from one dietary change. Prioritizing protein, healthy fats, and non-starchy vegetables supports the same mechanism.
5. Can metabolic syndrome be reversed?
Yes. Metabolic syndrome is a reversible metabolic state, not a permanent diagnosis. Because all five criteria share the same upstream driver — insulin resistance — interventions that address insulin resistance improve all five markers simultaneously. Carbohydrate restriction, resistance and aerobic exercise, quality sleep, and visceral fat reduction have all demonstrated measurable improvements in the full diagnostic cluster in clinical trials. The research is consistent: early-stage metabolic syndrome responds strongly to targeted dietary intervention.
6. How common is metabolic syndrome in the United States?
Approximately one in three American adults — roughly 35% — meets the clinical criteria for metabolic syndrome, according to NHANES data analyzed in a 2015 JAMA study by Aguilar and colleagues. Prevalence increases significantly with age, exceeding 50% in adults over 60. Most people who meet the criteria are unaware, because the condition produces no single obvious symptom and standard annual physicals rarely assess all five markers simultaneously.
Sources
Aguilar M et al. — "Prevalence of the Metabolic Syndrome in the United States, 2003–2012" (JAMA, 2015)
https://pubmed.ncbi.nlm.nih.gov/25988468/
Grundy SM et al. — "Diagnosis and Management of the Metabolic Syndrome" (Circulation, 2005)
https://pubmed.ncbi.nlm.nih.gov/16157765/
Meng Y et al. — "Efficacy of low carbohydrate diet for type 2 diabetes mellitus management" (Diabetes Research and Clinical Practice, 2017)
https://pubmed.ncbi.nlm.nih.gov/28750216/
Gami AS et al. — "Metabolic syndrome and risk of incident cardiovascular events and death" (JACC, 2007)
https://pubmed.ncbi.nlm.nih.gov/17258085/
Eckel RH et al. — "The metabolic syndrome" (Lancet, 2005)

Let Me See The Ai Audit Report
I had the MAP30 course material audited and graded by 4 dirrerent Ai models. I was shocked by the grade. See what they had to say about the MAP30 course.
Jaabsha Marketing LLC | All rights reserved 2024 Terms Of Service