Edition: Insulin & Blood Sugar
10 March, 2026
In The News
Vol 1, Edition 6
What Is Insulin Resistance — The Hidden Driver Behind Weight Gain and Metabolic Disease
You don't need a diabetes diagnosis to have insulin resistance. Millions of Americans are living with it right now — tired, foggy, struggling to lose weight, and getting the wrong answer from their doctor because nobody checked the right thing. Here's what insulin resistance actually is, how to recognize it, and what the evidence says about reversing it.

Published By: MAP30 Challenge
Authored By: John Shaw
12.2%
of American adults have optimal metabolic health
Araújo et al., UNC / NHANES 2009–2016
~40%
of adults 18–44 are insulin resistant, per HOMA-IR measurement
NHANES 2021 / StatPearls
96M+
American adults have prediabetes — 80% are unaware
CDC National Diabetes Statistics Report 2024
A Scenario That Plays Out Every Day
A common assumption — embedded in mainstream medical advice for decades — is that insulin resistance is simply the result of overeating and not exercising enough: a lifestyle choice with a lifestyle fix. The biology is more specific than that. Insulin resistance is a measurable hormonal condition driven primarily by the composition of the diet, not just its quantity — and understanding the distinction is the difference between managing symptoms and addressing the actual cause.
You are not unwell in any way you can name. You are tired, but you are busy. You have gained some weight around your midsection, but so has almost everyone you know. You get brain fog in the afternoon and need caffeine to close the gap. You sleep, but it is not restful. You crave sugar and refined carbohydrates in a way that feels less like preference and more like necessity.
You go to the doctor. Your fasting glucose is 99 — just below the prediabetes threshold of 100. Your doctor tells you everything looks fine.
What your doctor did not check — because most physicians do not, as a routine matter — is your fasting insulin level. That number, combined with your fasting glucose, would produce a HOMA-IR score: a well-established clinical measure of insulin resistance. And if that score were elevated, it would explain every symptom described above.
Insulin resistance does not announce itself with a clear diagnosis until it has been progressing for years, often decades. By the time a patient receives a prediabetes or type 2 diabetes diagnosis, the underlying metabolic dysfunction is not new. It is simply finally measurable by the thresholds medicine uses to trigger a formal label.
Understanding insulin resistance before that point — what it is, what drives it, and what reverses it — is the kind of metabolic literacy that most people never receive. This article is an attempt to change that.

What Insulin Resistance Actually Is
Insulin is the hormone produced by the beta cells of the pancreas in response to rising blood glucose. When you eat carbohydrates, they are broken down into glucose, which enters the bloodstream. Rising blood glucose is the signal for the pancreas to release insulin.
Insulin then circulates through the body and binds to receptors on cells — primarily in the liver, skeletal muscle, and adipose tissue — signaling them to take in glucose from the blood and either use it for energy or store it.
In a healthy metabolic state, this system is efficient and self-regulating. Glucose rises, insulin is released, cells respond, glucose is cleared, insulin levels fall. The cycle completes cleanly.
Insulin resistance is what happens when that signaling becomes impaired.
Cells — particularly in the liver, muscle, and fat tissue — stop responding normally to insulin's signal. The door is there, but the key no longer turns it as easily. The pancreas, sensing that glucose is not being cleared from the bloodstream, responds by producing more insulin. More insulin is released to achieve the same effect.
“Think of it as a lock that has become stiff over time. The key still fits, but you have to force it. And eventually, if you keep forcing it, the lock — and the mechanism behind it — starts to wear out.”
This compensatory hyperinsulinemia — chronically elevated insulin — is both a response to insulin resistance and a driver of it. High insulin levels suppress fat burning, because insulin's primary signal is to store energy, not release it. The body becomes locked in a state where it cannot easily access stored fat for fuel, regardless of what the scale says or how little the person is eating.
Over time, if the underlying causes are not addressed, the pancreas struggles to keep up with demand. Beta cell function declines. Blood glucose begins to rise more persistently. Prediabetes is diagnosed when fasting glucose reaches 100–125 mg/dL, or A1C reaches 5.7–6.4%. Type 2 diabetes is diagnosed when fasting glucose exceeds 126 mg/dL or A1C reaches 6.5% or higher.
But it is important to understand: the diagnosis of prediabetes or diabetes does not mark the beginning of the problem. It marks the point at which the problem has progressed far enough to cross a clinical threshold. The metabolic dysfunction — the insulin resistance itself — began years or decades before the label.
How Common Is It — and Why Most People Don't Know They Have It
The numbers on insulin resistance and metabolic health in the United States are difficult to absorb at face value, because they describe something far more widespread than most people's intuitions about disease prevalence would suggest.
A 2019 study from the University of North Carolina at Chapel Hill, published in Metabolic Syndrome and Related Disorders, analyzed NHANES data from 8,721 U.S. adults and found that only 12.2% met the criteria for optimal metabolic health — defined as having optimal levels of fasting glucose, blood pressure, triglycerides, HDL cholesterol, and waist circumference, without medication. That means roughly 88 out of every 100 adults fall short on at least one of those measures.
On insulin resistance specifically: a 2021 NHANES analysis cited by StatPearls (the NIH's clinical reference database) found that approximately 40% of U.S. adults aged 18 to 44 — a population traditionally considered low-risk — meet HOMA-IR criteria for insulin resistance. The condition is not confined to people who are obese or middle-aged. Half of those found to be insulin resistant in that study were not obese.
The problem is that standard blood tests — including fasting glucose and A1C — can appear normal for years while insulin resistance is already driving metabolic damage. The fasting insulin test catches the dysfunction early, before the standard markers move.
And yet most of these people have never been told. Fasting insulin is not part of a standard blood panel. HOMA-IR is not routinely calculated. The tests that would identify insulin resistance before it progresses to prediabetes are not standard-of-care screening tools in most clinical settings.
The result is a large population of people experiencing the consequences of insulin resistance — fatigue, weight gain, carbohydrate cravings, sleep disruption, cognitive fog — without any clinical framework to understand what is happening or why.
THE SIGNS THAT ARE EASY TO MISS
Visceral fat accumulation — weight carried around the abdomen and internal organs
Fatigue after meals, particularly after carbohydrate-heavy foods
Brain fog, difficulty concentrating, especially in the afternoon
Poor or non-restorative sleep
Persistent carbohydrate and sugar cravings that feel physiological, not just habitual
Skin tags — benign but associated with insulin resistance in clinical literature
Acanthosis nigricans — darkened, velvety skin in folds of the neck, armpits, or groin
Difficulty losing weight despite calorie restriction
Fasting glucose in the high-normal range (90–99 mg/dL), even without a prediabetes diagnosis
None of these signs individually confirms insulin resistance. But in combination — particularly with a high-normal fasting glucose and a diet high in refined carbohydrates — they represent a clinical picture that warrants further investigation. The appropriate test is a fasting insulin level alongside a fasting glucose, which allows a HOMA-IR score to be calculated. This is a simple blood test that most labs can perform; it simply is not ordered unless you or your physician asks for it.
What Drives Insulin Resistance: The Dietary Mechanism
Insulin resistance is a multifactorial condition — genetics, physical activity, sleep quality, chronic stress, and visceral fat all play roles. But the primary driver, in the context of modern Western dietary patterns, is the chronic overconsumption of rapidly digestible carbohydrates: refined grains, added sugars, and ultra-processed foods whose carbohydrate content is engineered to absorb quickly.
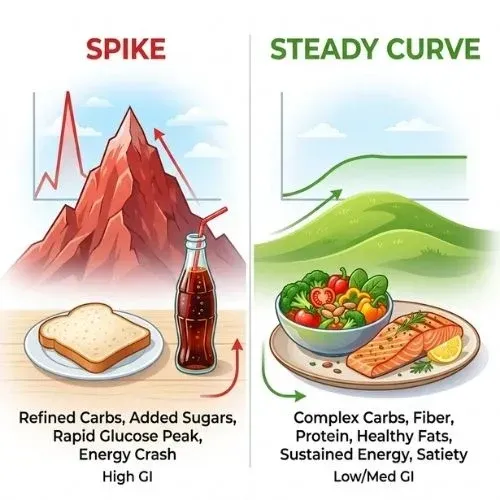
Here is the mechanism in plain terms. Carbohydrates are broken down into glucose during digestion. The speed of that breakdown determines how fast glucose enters the bloodstream — the glycemic response. Refined carbohydrates, stripped of fiber and processed to absorb rapidly, produce sharp, high blood glucose spikes. Those spikes trigger large, rapid insulin releases. Fiber-rich whole foods produce slower, more gradual glucose curves and correspondingly lower insulin demand.
When high-glycemic eating is the daily pattern — as it has been for a large portion of the American population for decades, partly as a consequence of the low-fat dietary guidelines that replaced fat with refined carbohydrate — the insulin system is under near-constant demand. Insulin levels remain chronically elevated. Cells, exposed to persistent high insulin signaling, progressively downregulate their response. Insulin resistance develops gradually, typically over years.
There is an important nuance worth understanding about the glycemic index. It is sometimes used as a shorthand for "foods that spike blood sugar," but the more clinically relevant concept is glycemic load — which accounts for both a food's glycemic index and the amount consumed. White bread, for instance, has a glycemic index comparable to or higher than table sugar, because the starch in highly refined white bread is broken down and absorbed very rapidly. Two slices of white bread can produce a blood glucose response comparable to several teaspoons of pure sugar — not because of their sugar content as listed on a label, but because of how fast the refined starch converts to glucose in the digestive tract.
| Dietary Factor | Effect on Insulin and Metabolic Health |
|---|---|
| Refined carbohydrates (white bread, white rice, processed cereals) | Rapid glucose absorption → large insulin spike → chronically elevated insulin demand over time. |
| Added sugar and HFCS | Fructose component processed by liver → de novo lipogenesis → liver fat → worsens hepatic insulin resistance. |
| Ultra-processed foods | Engineered for rapid absorption; often combine refined carbs and fats in ratios that maximize insulin response and override satiety signaling. |
| Dietary fiber (vegetables, legumes, whole grains) | Slows glucose absorption → blunts insulin response → supports insulin sensitivity over time. |
| Protein | Minimal direct insulin impact at moderate intake; supports muscle mass, which is the primary site of glucose disposal and a key driver of insulin sensitivity. |
| Healthy fats (olive oil, nuts, avocado, fatty fish) | Lowest glycemic impact of any macronutrient; associated with improved insulin sensitivity in clinical research. |
The Downstream Consequences: Why Insulin Resistance Is the Upstream Problem
Insulin resistance is not simply a precursor to diabetes. It is a systemic metabolic disruption with documented associations across a wide range of chronic conditions — which is why researchers increasingly describe it as the central driver of what is broadly called metabolic syndrome.
The downstream consequences of chronic insulin resistance and hyperinsulinemia include:
Type 2 diabetes: The most direct downstream consequence. As insulin resistance worsens and the pancreas struggles to compensate, blood glucose rises persistently into the diabetic range.
Cardiovascular disease: Chronic hyperinsulinemia promotes arterial inflammation, raises triglycerides, lowers HDL cholesterol, and drives hypertension — all independent cardiovascular risk factors.
Non-alcoholic fatty liver disease (NAFLD): Insulin resistance in the liver drives de novo lipogenesis — the conversion of excess glucose and fructose into liver fat. NAFLD is now the most common chronic liver disease in the United States and is directly linked to insulin resistance.
Obesity and difficulty losing weight: High insulin suppresses lipolysis — the release of stored fat for fuel. A person with significant insulin resistance can be in a calorie deficit and still struggle to access stored body fat effectively, because the hormonal environment keeps the body locked in fat storage mode.
Polycystic ovary syndrome (PCOS): Insulin resistance is present in an estimated 50–70% of women with PCOS and is considered a primary driver of the hormonal dysregulation that characterizes the condition.
Cognitive decline: Emerging research has characterized Alzheimer's disease as a condition with features of insulin resistance in the brain — sometimes informally described as "type 3 diabetes" in research contexts — with hyperinsulinemia associated with impaired glucose metabolism in brain tissue.
This breadth of downstream consequence is why insulin resistance is increasingly described not as a single disease precursor but as the common metabolic root of a cluster of the most prevalent chronic conditions in the Western world. Addressing it upstream — before the downstream diagnoses accumulate — is substantially more effective than treating each condition individually after the fact.
Is Insulin Resistance Reversible? What the Evidence Shows
The answer supported by current clinical research is yes — for most people, and particularly for those who have not yet progressed to full type 2 diabetes, insulin resistance is a reversible condition. The mechanisms that drive it are dietary and lifestyle in nature, which means the interventions that reverse it are also dietary and lifestyle in nature.
The most direct lever is reducing the chronic carbohydrate and insulin load that drives the condition in the first place. When dietary carbohydrates — particularly refined carbohydrates and added sugar — are reduced, blood glucose fluctuations become smaller, insulin demand decreases, chronically elevated insulin levels fall, and cells progressively restore their sensitivity to insulin signaling.
This is the direct mechanism behind stubborn fat that doesn't respond to calorie restriction — and understanding how the body switches between fat storage and fat burning mode changes the entire approach to weight loss.
This does not require extreme dietary restriction. The clinical research points to several specific interventions with consistent evidence:
| Intervention | What the Evidence Supports |
|---|---|
| Reduce refined carbohydrates and added sugar | The most direct dietary lever. Lowering carbohydrate intake reduces the insulin demand that drives resistance. Multiple clinical trials show measurable improvements in fasting insulin and HOMA-IR within weeks. |
| Prioritize protein and dietary fiber | Protein supports muscle mass — the primary site of glucose disposal. Fiber blunts glucose absorption and feeds gut bacteria associated with improved insulin sensitivity. |
| Time-restricted eating / intermittent fasting | Extending the daily fasting window (e.g., 12–16 hours) allows insulin levels to drop for sustained periods, creating the hormonal conditions in which fat oxidation and insulin sensitivity can recover. |
| Resistance and aerobic exercise | Skeletal muscle is the largest glucose sink in the body. Both resistance training and aerobic exercise acutely improve insulin sensitivity, independent of weight loss. Exercise is one of the most reliable insulin-sensitizing interventions in the literature. |
| Reduce visceral fat | Visceral fat — the fat that accumulates around internal organs — is metabolically active and a driver of systemic insulin resistance. Weight loss that specifically reduces visceral fat produces measurable improvements in insulin sensitivity. |
| Improve sleep quality and duration | Even a single night of poor sleep produces measurable increases in insulin resistance. Chronic sleep deprivation is an independent driver of metabolic dysfunction. Addressing sleep is not optional in any serious effort to reverse insulin resistance. |
The timeline for measurable improvement varies considerably by individual, by the severity of insulin resistance, and by how consistently the interventions are applied. Some people see measurable changes in fasting insulin and blood glucose within 2 to 4 weeks of meaningful dietary change. For others, particularly those with longer-standing metabolic dysfunction, meaningful improvement may take months. What the evidence consistently shows is that the direction of change — restoration of insulin sensitivity — is achievable through non-pharmacological means for the majority of people with insulin resistance that has not yet progressed to advanced type 2 diabetes.
“The same mechanisms that drove insulin resistance — years of high carbohydrate intake and chronically elevated insulin — are the same levers that reverse it, applied in the opposite direction. The biology is not permanent. The condition is not a life sentence.”
What to Ask Your Doctor: Getting the Right Tests
Standard blood panels do not routinely include the tests that identify insulin resistance before it reaches the prediabetes or diabetes threshold. If you recognize the signs described in this article, or if your fasting glucose is in the high-normal range (90–99 mg/dL), the following tests are worth discussing with your physician:
TESTS WORTH REQUESTING
Fasting insulin — this, combined with fasting glucose, allows HOMA-IR to be calculated. A HOMA-IR of 2.0 or higher is generally associated with insulin resistance, though lab reference ranges vary.
Fasting glucose — standard but interpreted more usefully alongside fasting insulin.
Hemoglobin A1C — a 3-month average of blood glucose; a better chronic marker than a single fasting glucose reading.
Triglycerides and HDL cholesterol — a triglyceride-to-HDL ratio above 3.0 is an accessible proxy marker for insulin resistance in the absence of direct insulin testing.
Waist circumference — greater than 40 inches in men and 35 inches in women is a recognized risk criterion for metabolic syndrome. This costs nothing and takes 30 seconds.
If your physician is unfamiliar with HOMA-IR or does not routinely order fasting insulin, it is entirely reasonable to request it directly. The test is widely available, inexpensive, and provides substantially more metabolic information than fasting glucose alone. A proactive conversation about metabolic screening — particularly if you have multiple signs described in this article — is an appropriate and well-supported clinical discussion.
Bottom Line
Insulin resistance is arguably the most consequential and most underdiagnosed metabolic condition in the United States. Its prevalence is not limited to people who are obese, elderly, or visibly unwell. It is present in an estimated 40% of young adults. It precedes virtually every major chronic metabolic disease. And it develops silently — over years, sometimes decades — before it crosses any clinical threshold that triggers a formal diagnosis.
The signs are real and recognizable. The mechanisms are well understood. The interventions that reverse it are available to most people without a prescription. And the window for intervention — between the first signs of metabolic dysfunction and a diagnosis that requires medication — is where the most meaningful change is possible.
The first step is metabolic literacy: understanding that a fasting glucose of 97, combined with persistent fatigue, abdominal weight gain, and carbohydrate cravings, is not a clean bill of health. It is a picture worth looking at more carefully. The tests exist. The interventions are grounded in evidence. The direction of change is achievable.
What most people with insulin resistance have never been given is the framework to understand what is happening in their own body. That framework is not complicated. It starts with knowing that insulin — not just calories, not just fat — is the central metabolic signal that determines whether you store energy or burn it. And that the foods you eat, every single day, are either supporting that system or slowly degrading it.
Key references: Araújo J, Cai J, Stevens J, "Prevalence of Optimal Metabolic Health in American Adults" (Metabolic Syndrome and Related Disorders, 2019); Freeman AM, Acevedo LA, Pennings N, "Insulin Resistance" (StatPearls / NCBI, updated 2023); Parcha V et al., "Insulin Resistance and Cardiometabolic Risk Profile Among Nondiabetic American Young Adults" (Journal of Clinical Endocrinology and Metabolism, 2022); CDC National Diabetes Statistics Report (2024); Taylor R, "Type 2 Diabetes: Etiology and Reversibility" (Diabetes Care, 2013); Kolb H et al., "Environmental/lifestyle factors in the pathogenesis and prevention of type 2 diabetes" (BMC Medicine, 2017).
This article is part of our Insulin & Blood Sugar series.
Link Here: Insulin & Blood Sugar
Latest Articles
California Lawsuit
A first-of-its-kind lawsuit filed on behalf of the People of California accuses the country's largest food companies of knowingly engineering...

Type 2 Diabetes
In 2021, an international expert group convened by the American Diabetes Association — alongside the European Association for the Study of Diab...

Scale Stopped Moving?
Calories don't control your weight. Hormones do. And once you understand the difference, everything changes...

John Shaw
MAP30 Challenge
John Shaw is a Certified Nutrition Educator and the founder of the MAP30 Challenge. What began as a personal health journey at 294 pounds, and pre-diabetic, evolved into a structured 30-day metabolic reset program grounded in nutritional science. John's mission is simple: give people the biological education that the diet industry never did.
⚠ Disclaimer
The information in this article is for educational purposes only and does not constitute medical advice. Insulin resistance and related metabolic conditions are serious health matters. Nothing in this article should be interpreted as a recommendation to change, stop, or start any medication, diet, or treatment plan. Always consult a qualified healthcare provider before making changes to how you manage your health. Individual results vary.
FAQ's
1. What is insulin resistance?
Insulin resistance is a metabolic condition in which the body's cells stop responding normally to insulin — the hormone the pancreas produces to move glucose from the bloodstream into cells for energy. When cells become resistant, the pancreas compensates by producing more insulin. Over time, chronically elevated insulin promotes fat storage, inflammation, and a cascade of metabolic dysfunction that precedes type 2 diabetes by years or decades.
2. What causes insulin resistance?
The primary dietary driver is chronic consumption of refined carbohydrates, added sugars, and ultra-processed foods — which repeatedly spike blood glucose and keep insulin elevated. Other contributors include physical inactivity, chronic sleep deprivation, chronic psychological stress, excess visceral fat, and genetic predisposition. Insulin resistance and leptin resistance typically develop together and reinforce each other.
3. What are the symptoms of insulin resistance?
Common signs include: difficulty losing weight especially around the abdomen, energy crashes after meals, strong carbohydrate and sugar cravings, brain fog, skin tags or dark patches of skin (acanthosis nigricans), elevated fasting blood glucose, high triglycerides, low HDL cholesterol, and high blood pressure. Many people have insulin resistance for years before it shows up on standard blood tests.
4. How do you test for insulin resistance?
The most sensitive early test is a fasting insulin level — ideally below 5 mIU/L, with levels above 10 a strong indicator of resistance. Standard fasting blood glucose misses early insulin resistance because glucose can appear normal while insulin is chronically elevated. The HOMA-IR score, calculated from fasting glucose and fasting insulin, provides a more accurate picture of insulin sensitivity.
5. Can insulin resistance be reversed?
Yes — insulin resistance is largely reversible through dietary and lifestyle changes, particularly in its earlier stages. The most effective interventions are: reducing refined carbohydrates and added sugars to lower chronic insulin elevation; increasing whole food protein and healthy fats; regular physical activity especially resistance training; prioritizing sleep; and managing chronic stress. Many people see measurable improvements in fasting insulin within weeks of consistent dietary change.
6. How does insulin resistance cause weight gain?
Chronically elevated insulin promotes fat storage and simultaneously prevents fat burning — you cannot burn stored fat and have high insulin at the same time. Additionally, insulin resistance disrupts leptin signaling, causing the brain to think the body is starving even when fat stores are full. This drives increased hunger, slows metabolism, and creates a biological environment in which weight loss is working against the body's own hormonal programming.
Sources
Reaven GM — 'Banting lecture 1988: Role of insulin resistance in human disease' (Diabetes, 1988)
https://pubmed.ncbi.nlm.nih.gov/3056758/
Crofts CAP et al. — 'Hyperinsulinemia: A unifying theory of chronic disease?' (Diabesity, 2015)
https://pubmed.ncbi.nlm.nih.gov/26756000/
Westman EC et al. — 'Low-carbohydrate nutrition and metabolism' (Am J Clin Nutr, 2007)
https://pubmed.ncbi.nlm.nih.gov/17684196/
Lustig RH — 'Fructose: metabolic, hedonic, and societal parallels with ethanol' (JADA, 2010)
https://pubmed.ncbi.nlm.nih.gov/20869486/
Kraft JR — 'Diabetes Epidemic and You' (Trafford Publishing, 2008)

Let Me See The Ai Audit Report
I had the MAP30 course material audited and graded by 4 dirrerent Ai models. I was shocked by the grade. See what they had to say about the MAP30 course.
Jaabsha Marketing LLC | All rights reserved 2024 Terms Of Service