Edition: Weight Loss & Fat Burning
26 February, 2026
In The News
Vol 1, Edition 5
You're In a Calorie Deficit and Still Not Losing Weight? Here's Why.
The calorie deficit model has been the foundation of weight loss advice for over a century. But millions of people follow it precisely — and still get nowhere. The problem isn't your discipline. The problem is that the model is incomplete. Here's what the science actually says.

Published By: MAP30 Challenge
Authored By: John Shaw
25%
potential drop in BMR with chronic calorie restriction
~30%
fewer calories fiber-rich foods may actually deliver vs. label
1958
year the 3,500 cal = 1 lb rule was derived from limited data
~75%
of calorie burn comes from sources other than exercise
The Rule Everyone Follows — And Why It Keeps Failing
You've probably heard it a thousand times: eat less, move more. Create a calorie deficit. Lose weight. The math is simple. The physics is airtight. And yet, for millions of people who do exactly this, the scale doesn't move.
That's not a failure of willpower. That's a failure of an incomplete model being sold as a complete one. The calorie deficit framework captures one real truth — the law of thermodynamics — and then ignores everything else that actually governs how your body stores and burns fuel. Why that model keeps failing — and why the diet industry has built a billion-dollar business on that failure — starts with understanding what actually controls fat storage.
To understand why it breaks down, you first need to understand where it came from — and what assumptions were baked in from the very beginning.
The 19th Century Science Still Running Your Nutrition Label
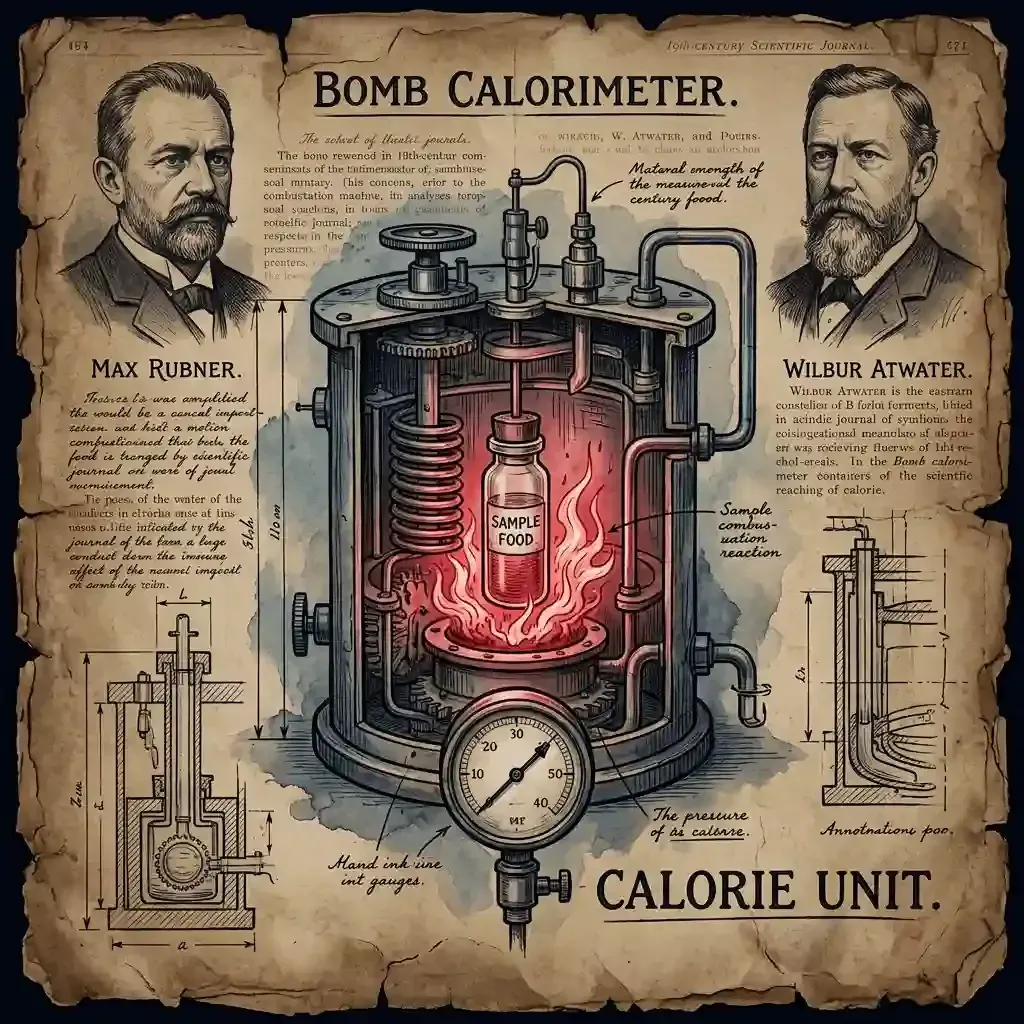
The calorie model has two founding fathers, and neither of them was studying living humans when they built it.
In the 1880s, German physiologist Max Rubner applied the laws of thermodynamics to human metabolism. He used a device called a bomb calorimeter — a sealed chamber that literally burns food and measures the heat released. That heat measurement became the calorie. The problem: a bomb calorimeter is a closed system. A furnace burning food in a lab and a human digestive system are not the same thing.
Then came U.S. chemist Wilbur Atwater in the 1890s.
He refined Rubner's work and created what's now called the Atwater system — the formula that still powers every nutrition label in America today. Atwater assigned fixed calorie values: carbohydrates at 4 calories per gram, protein at 4 calories per gram, fat at 9 calories per gram. He calculated these values by measuring how much heat food produced when burned outside the body — and then assumed the body used these fuels with similar efficiency.
I
"That assumption — that the human body burns fuel like a furnace — is the crack in the foundation that the entire calorie model was built on.
The law of thermodynamics itself is not wrong. Applied to the body, it says: Energy In (food) = Energy Stored (fat and glycogen) + Energy Out (heat, movement, organ function). That's mathematically true. The critical question the model fails to answer is: what controls the 'Energy Out' side of that equation? And the answer, it turns out, is your hormones — not your calculator.
What 'Calories Out' Actually Means — The Part Nobody Explains
Most people hear 'calories out' and think: exercise. Burn more at the gym, lose more weight. But exercise is actually the smallest piece of the energy expenditure puzzle. Your total daily energy expenditure (TDEE) is made up of four distinct components — and only one of them is your workout.
| Component | What It Is & Why It Matters |
|---|---|
| BMR — Basal Metabolic Rate | The calories your body burns just to stay alive — breathing, circulation, organ function. This accounts for roughly 60–70% of total calorie burn and is the component most affected by chronic calorie restriction. |
| TEF — Thermic Effect of Food | The energy it takes to digest and process what you eat. Protein has the highest TEF (20–30%), meaning your body burns more calories processing protein than carbs or fat. |
| NEAT — Non-Exercise Activity Thermogenesis | All movement that isn't formal exercise — fidgeting, walking to the car, standing, gesturing. This is highly variable and is one of the first things your body reduces when calories drop. |
| EAT — Exercise Activity Thermogenesis | Actual intentional exercise. Despite being the focus of most weight loss advice, this typically accounts for only 5–15% of total daily calorie burn. |
Why does this breakdown matter? Because when you cut calories, your body doesn't just sit there — it responds by cutting calories out. Every component on that list is subject to downward adjustment when the body senses an energy deficit. That response has a name.
When you chronically restrict calories, your body interprets it as a threat to survival. It doesn't know you're trying to fit into last year's jeans. It responds the same way it has for millions of years of human evolution: it becomes more efficient.
BMR can drop by 15 to 25% during periods of sustained calorie restriction. Your body literally turns down the thermostat on basic functions to preserve stored energy. NEAT drops in parallel — you unconsciously move less, fidget less, feel more fatigued. The combined effect is that you eat less AND burn less, until the deficit you created on paper has effectively closed in your body.
This is sometimes called 'starvation mode' — though that term gets overused. The more precise term is metabolic adaptation, and it's well-documented in the research. It's not a myth, and it's not an excuse. It's your body doing exactly what it evolved to do.
I
"The result: you eat less, your body burns less. The deficit you calculated disappears. And then everyone tells you to try harder.
The Label Lie: Your Calorie Count Is Already Wrong
Even if metabolic adaptation wasn't an issue, the calorie math most people are using is based on numbers that don't hold up under modern scrutiny.
The Atwater system — again, from the 1890s — assigns fixed calorie values to macronutrients. But contemporary research has shown that actual calorie availability varies significantly depending on the food's structure, processing level, and your individual gut microbiome.
Where the Numbers Break Down
Fiber-rich foods may deliver 20–30% fewer usable calories than their labels suggest, because fiber resists digestion and passes through the gut largely intact
Processing dramatically increases calorie availability — a raw almond and almond butter made from those same almonds are not metabolically equivalent, even if the label says otherwise
Two people eating the exact same meal can absorb meaningfully different amounts of calories, depending on the composition of their gut microbiome
The 3,500 calorie = 1 pound rule — the equation behind virtually every weight loss projection ever given — was derived from a single 1958 paper by Max Wishnofsky, based on extremely limited data. It was never meant to be a precise formula, and decades of research have confirmed it doesn't hold up in practice
The implication is uncomfortable but important: even if you're meticulously tracking every calorie in and every calorie burned, the numbers you're working with have a significant margin of error built in from the start.
Insulin: The Hormone the Calorie Model Ignores
This is where the calorie deficit model doesn't just fall short — it actively misleads people. Because the most powerful driver of fat storage and fat burning in the human body isn't calories. It's insulin.
Insulin is the storage hormone. When insulin levels are elevated, your body is in store mode. Fat burning is suppressed. The body prioritizes moving glucose and nutrients into cells — and when those cells are already full, into fat tissue. This is normal and healthy in the short term. The problem is what happens when the system breaks down.
In insulin resistance — which is far more common than most people realize and often goes undiagnosed for years — cells stop responding normally to insulin signals. The pancreas compensates by pumping out more insulin. The result is chronically elevated insulin levels, even in a fasted state.
This is why two people can eat identical 1,500-calorie diets and get completely different results. Their calorie math is the same. Their hormonal environment is not.
I
"High insulin = body locked in storage mode. Even when calories are low, the hormonal signal says: hold the fat. CICO doesn't account for this at all.
And here's the part that makes standard diet advice actively counterproductive for people with insulin resistance: cutting calories the conventional way — reducing fat, leaning on 'low calorie' carbohydrates, eating frequent small meals — can keep insulin elevated and make fat loss physiologically harder, not easier.
How Cutting Calories Can Make Things Worse
This is one of the most important and least-discussed aspects of the calorie deficit model. For a significant portion of the population, following standard advice doesn't just fail to produce results — it creates a hormonal environment that actively works against fat loss.
The Cascade Nobody Warns You About
Chronic under-eating raises cortisol, the primary stress hormone. Elevated cortisol directly drives blood sugar up — which drives insulin up, reinforcing storage mode
Traditional calorie cutting typically means reducing dietary fat and increasing carbohydrates ('low fat = low calorie'). But carbohydrates are the primary driver of insulin secretion. More carbs means more insulin — the opposite of what someone with insulin resistance needs
Calorie restriction triggers a measurable increase in ghrelin (the hunger hormone) and a drop in leptin (the satiety hormone). This creates a physiological drive to eat that has nothing to do with willpower — it's a hormonal response to perceived starvation
Muscle mass, which is metabolically expensive and one of the most important factors in long-term metabolic health, tends to be lost alongside fat during aggressive calorie restriction — further lowering BMR
The cycle is vicious and self-reinforcing: eat less, cortisol rises, insulin stays high, fat burning stays suppressed, hunger intensifies, you eat more, you blame yourself. Repeat.
What Actually Moves the Needle
The goal isn't to abandon the idea of energy balance — it's real, and it matters. The goal is to fix the hormonal environment that controls what your body actually does with the energy it receives. When insulin resistance is addressed, the body can begin accessing stored fat again — often without the aggressive calorie restriction that triggers metabolic adaptation.
This doesn't mean calories are irrelevant. It means that for many people, getting the hormonal environment right is the prerequisite that makes everything else work.
Three Foundational Shifts to Consider
| Shift | The Logic Behind It |
|---|---|
| Prioritize protein at every meal | Protein has the highest thermic effect of any macronutrient, supports muscle retention during a deficit, and has a minimal impact on insulin compared to refined carbohydrates. It also drives satiety more effectively than carbs or fat. |
| Reduce refined carbohydrates before reducing total calories | For people with insulin resistance, cutting the foods that spike insulin most aggressively — sugar, refined grains, liquid calories — often produces better fat loss results than calorie counting, even without a significant reduction in total intake. |
| Incorporate time-restricted eating | Extending the overnight fast (even to 12–14 hours) gives insulin levels time to drop, which opens the window for fat oxidation. This has nothing to do with calories — it's about creating sustained low-insulin periods. |
The Bottom Line
The calorie deficit model isn't wrong. It's incomplete. It captures a real law of physics and then ignores the biological machinery that actually executes that law inside a living human body. The process of how fat is accumulated and burns fat is complex and goes far beyond the simplicity it's made out to be.
If you've been eating at a deficit, tracking every bite, doing everything right by the conventional rulebook — and still not losing weight — you are not broken. You are not lacking discipline. You are likely dealing with metabolic adaptation, hormonal dysregulation, or both. And the solution isn't to eat less. It's to understand what's actually happening and address it at the source.
I
You're not failing the diet. The diet is failing to account for your biology.
The science on insulin resistance, metabolic adaptation, and hormonal drivers of fat storage is growing fast. The standard advice hasn't caught up yet. But understanding these mechanisms — and sharing them — is how that starts to change.
Key references: Atwater System (1890s); Wishnofsky M., Caloric equivalents of gained or lost weight (1958); Hall KD et al., Quantification of the effect of energy imbalance on bodyweight (Lancet, 2011); Rosenbaum M & Leibel RL, Adaptive thermogenesis in humans (Int J Obesity, 2010).
This article is part of our Weight Loss & Fat Burning series. Weight Loss & Fat Burning

Latest Articles

Insulin Resistance
You don't need a diabetes diagnosis to have insulin resistance. Millions of Americans are living with it right now...

How Mitochondria Work
Persistent fatigue, mid-morning crashes, brain fog, and poor sleep are not personality traits or signs of aging. They are symptoms...

Type 2 Diabetes
In 2021, an international expert group convened by the American Diabetes Association — alongside the European Association for the Study of Diab...

John Shaw
MAP30 Challenge
John Shaw is a Certified Nutrition Educator and the founder of the MAP30 Challenge. What began as a personal health journey at 294 pounds, and pre-diabetic, evolved into a structured 30-day metabolic reset program grounded in nutritional science. John's mission is simple: give people the biological education that the diet industry never did.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Individual results vary. Always consult your healthcare provider before making dietary changes, especially if you have a medical condition or take medications.
FAQ's
1. Why am I not losing weight even in a calorie deficit?
The most likely explanation is metabolic adaptation — your body has responded to reduced calorie intake by lowering the amount of energy it burns. BMR (your baseline calorie burn) can drop by 15 to 25% during sustained calorie restriction, and NEAT (non-exercise movement) also decreases. This means the deficit you calculated on paper may no longer exist inside your body. Hormonal factors, particularly elevated insulin in people with insulin resistance, can also lock the body into storage mode even when calories are low. The short answer: eating less is not always enough, and for many people, the hormonal environment matters more than the calorie math.
2. How accurate are calorie counts on food labels?
Less accurate than most people realize. Food labels in the U.S. still use the Atwater system — a formula developed in the 1890s that assigns fixed calorie values to macronutrients based on how much heat food produces when burned outside the body. Modern research shows several gaps: fiber-rich foods may deliver 20–30% fewer usable calories than the label states; processing significantly increases calorie availability (a raw almond vs. processed almond butter are not metabolically equivalent); and individual gut microbiome differences mean two people can absorb different amounts from the exact same meal. The 3,500 calorie = 1 pound rule, still used in most weight loss calculators, was based on a single 1958 paper and has never been validated as a precise formula. The numbers on labels are useful estimates — not precise measurements of what your body will absorb.
3. What is metabolic adaptation and how do I fix it?
Metabolic adaptation is your body's survival response to calorie restriction. When calories drop, your body reduces how much energy it burns — lowering BMR, suppressing NEAT (unconscious daily movement), and altering hormones like leptin and ghrelin to increase hunger. The good news: research from the University of Alabama at Birmingham has shown that metabolic adaptation is not permanent. A short period of weight stabilization — even just two weeks of eating at maintenance calories — can significantly reduce or reverse it. From there, reintroducing a moderate deficit tends to produce better results than continued aggressive restriction. Prioritizing protein intake and resistance training are also well-supported strategies for limiting how much metabolic adaptation occurs during weight loss.
4. Does insulin affect weight loss?
Insulin is the primary storage hormone in the human body. When insulin levels are elevated, fat burning is suppressed — the body is in 'store mode.' In people with insulin resistance (estimated to affect around 40% of U.S. adults according to Yale School of Medicine research), insulin levels stay chronically elevated even in a fasted state, because cells aren't responding normally and the pancreas compensates by producing more. This can make fat loss physiologically difficult regardless of calorie intake. The Carbohydrate-Insulin Model of obesity, published in PMC, argues that for insulin-resistant individuals, reducing refined carbohydrates — which are the primary driver of insulin secretion — may be more effective for fat loss than simply cutting total calories.
5. Should I count calories or use a better approach?
Calorie awareness is useful — but calorie counting alone is an incomplete strategy for many people, particularly those dealing with metabolic adaptation, insulin resistance, or hormonal imbalances. A more effective framework focuses on the hormonal environment first: reducing refined carbohydrates to lower insulin, prioritizing protein to support muscle retention and satiety, and incorporating time-restricted eating to create sustained low-insulin windows that allow fat oxidation. Calories still matter in the background, but for people who have been stuck despite tracking precisely, addressing the hormonal drivers tends to produce results that calorie math alone cannot. Work with a healthcare provider if you suspect insulin resistance or have an underlying metabolic condition — these are medical issues, not discipline issues.
Sources
Adaptive Thermogenesis in Humans
International Journal of Obesity (Rosenbaum & Leibel)
https://www.nature.com/articles/ijo2010173
Quantification of the Effect of Energy Imbalance on Bodyweight
The Lancet
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(11)60812-X/fulltext
Calorie Restriction & Metabolism
Impact of Calorie Restriction on Energy Metabolism in Humans — PMC / NCBI
https://pmc.ncbi.nlm.nih.gov/articles/PMC9036397/
Insulin Resistance Research
Insulin Resistance and Obesity — StatPearls / NCBI
https://www.ncbi.nlm.nih.gov/books/NBK507839/
Thermic Effect of Food
Diet-Induced Thermogenesis — The American Journal of Clinical Nutrition
https://academic.oup.com/ajcn/article/89/1/197S/4596794
Atwater System
History of the Atwater System for Calorie Calculation — USDA
https://www.ars.usda.gov/ARSUserFiles/80400525/Data/Classics/atwater.pdf

Let Me See The Ai Audit Report
I had the MAP30 course material audited and graded by 4 dirrerent Ai models. I was shocked by the grade. See what they had to say about the MAP30 course.
Jaabsha Marketing LLC | All rights reserved 2024 Terms Of Service