Edition: Hormones & Metabolism
28 March, 2026
In The News
Vol 1, Edition 20
What Are Hormones and How Do They Work — The Metabolic Orchestra Behind Your Weight, Energy, and Health
Most people think about weight gain as a math problem — calories in versus calories out. The biology is more complex than that. Your body is run by a hormonal system that decides whether to store fat or burn it, whether to feel hungry or satisfied, whether to have energy or feel exhausted. Understanding how that system works is the first step to working with your biology instead of against it.
Published By: MAP30 Challenge
Authored By: John Shaw
For most of my adult life I approached my weight the same way most people do — as a math problem. Eat less, move more. Count the calories. I spent years trying to solve a hormonal problem with arithmetic, and I kept losing. What changed everything was understanding that the body does not respond to food as a calorie counter. It responds to food as a hormonal signal. Every meal triggers a cascade that determines what happens to the energy you just consumed — whether it gets burned for fuel, stored as fat, or used to rebuild tissue. Most diets try to manage the calories. The biology cares about the hormones.
Understanding how that hormonal system works — what the key hormones are, what drives them, and what happens when they get out of balance — is the foundation that makes every other piece of metabolic education make sense. This is where it starts.
"Your body is not a calorie calculator. It is a hormonal system. The hormones determine what the calories do — whether they fuel your cells, build your muscle, or get stored as belly fat."
What Are Hormones and How Do They Work
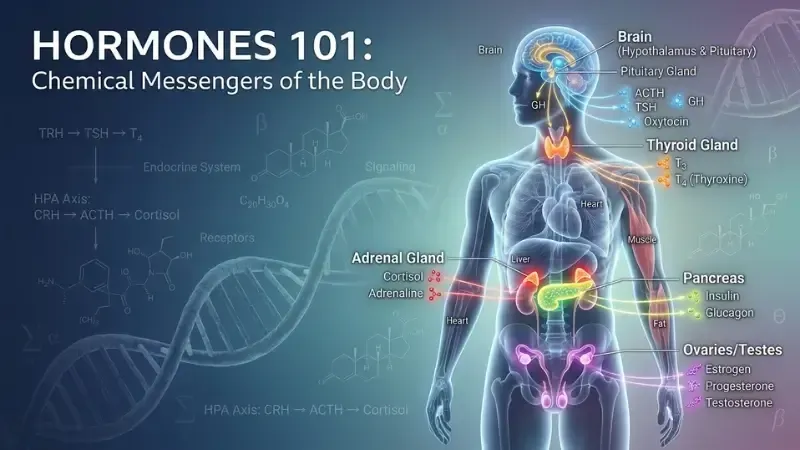
Hormones are chemical messengers produced by glands throughout the body that travel through the bloodstream and deliver instructions to cells, organs, and tissues. They regulate virtually every physiological process: metabolism, hunger, energy production, fat storage, sleep, stress response, reproduction, growth, and mood.
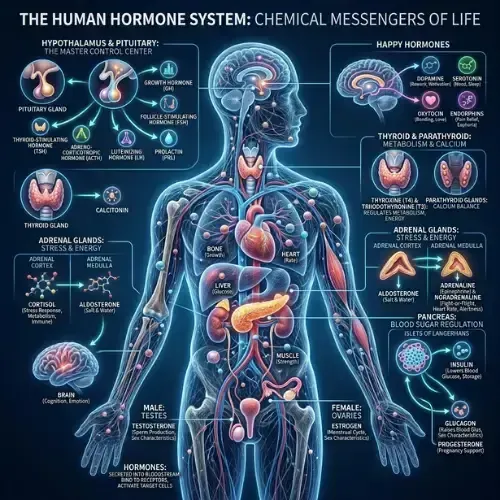
The endocrine system — the network of glands that produces and regulates hormones — includes the hypothalamus, pituitary gland, thyroid, adrenal glands, pancreas, and gonads. Each gland produces specific hormones in response to specific triggers, and those hormones travel through the blood to target cells equipped with receptors designed to receive them.
The relationship between a hormone and its receptor works like a lock and key. The hormone is the key; the receptor is the lock. When the key fits the lock, a signal is transmitted inside the cell that changes its behavior.
Insulin, for example, binds to insulin receptors on muscle and fat cells, signaling them to take up glucose from the blood. When cells stop responding to that signal — a condition called insulin resistance — the lock stops working even though the key is present. More and more insulin gets produced trying to force the door open, and the downstream consequences of that chronic overproduction are what drive metabolic disease.
Understanding how your metabolism works requires understanding the hormones that run it. The table below maps the primary metabolic hormones, where they come from, what triggers their release, and what they do:
| Gland / Source | Hormone | Release Trigger | Metabolic Role |
|---|---|---|---|
| Pancreas | Insulin | Blood glucose rises after eating | Drives glucose into cells; promotes fat storage; suppresses fat burning |
| Pancreas | Glucagon | Blood glucose falls; fasting state | Signals liver to release stored glucose; promotes fat burning |
| Adrenal Glands | Cortisol | Stress; sleep deprivation; low blood glucose | Raises blood glucose; promotes visceral fat storage; suppresses insulin sensitivity |
| Fat Cells | Leptin | Fat stores are adequate | Signals the brain to suppress hunger and increase energy expenditure |
| Stomach | Ghrelin | Fasting; caloric restriction; sleep deprivation | Stimulates hunger; promotes fat storage; rises when weight is lost |
| Thyroid | T3 / T4 | TSH from pituitary gland | Regulates metabolic rate, body temperature, and energy expenditure |
| Hypothalamus / Pituitary | GH (Growth Hormone) | Deep sleep; fasting; exercise | Promotes fat burning; builds lean muscle; stimulates cellular repair |
| Ovaries / Testes | Estrogen / Testosterone | Circadian and reproductive signals | Regulate fat distribution, muscle mass, bone density, and metabolic rate |
These hormones do not operate in isolation. They form an interconnected web of signals and feedback loops. Elevated insulin suppresses glucagon. Elevated cortisol raises blood glucose, which raises insulin. Sleep deprivation simultaneously elevates cortisol and ghrelin while suppressing leptin and growth hormone. Understanding this web — rather than any single hormone in isolation — is what makes metabolic health education genuinely useful.
Insulin — The Master Metabolic Hormone
Of all the metabolic hormones, insulin has the most direct and powerful effect on whether your body stores fat or burns it. Insulin is produced by the beta cells of the pancreas in response to rising blood glucose — primarily after eating carbohydrates and, to a lesser extent, protein. Its job is to move glucose out of the bloodstream and into cells.
But insulin does more than manage blood sugar. It is the primary fat-storage hormone. When insulin is elevated, the enzyme hormone-sensitive lipase — which initiates fat burning — is directly suppressed. Fat cells cannot release their stored fatty acids into the bloodstream for energy. The body is locked in storage mode regardless of how many calories you are consuming.
This is the mechanism behind the fundamental failure of calorie-restriction diets. If the dietary pattern keeps insulin chronically elevated — through frequent meals, refined carbohydrates, and added sugars — the hormonal environment for fat burning never fully establishes. You can eat less and still not access your fat stores because insulin is blocking the door.
In a controlled crossover study, participants on a low-carbohydrate diet burned 325 more calories per day during weight-loss maintenance than those on a low-fat diet at the same caloric intake — with the difference attributed to reduced insulin levels and improved fat oxidation. Dietary composition independently affects metabolic rate through hormonal mechanisms. (Ebbeling CB et al. — JAMA, 2012)
325 extra calories burned per day
on a low-carbohydrate diet vs low-fat diet at the same caloric intake — the difference driven entirely by insulin reduction
Ebbeling CB et al. — JAMA, 2012
What Hormones Block Weight Loss After 40
One of the most common experiences in metabolic health is doing everything right and still struggling to lose weight after 40. I see this consistently in the people who come through MAP30 — and I went through my own version of it. The biology behind this is real and specific. It is not about discipline failing. It is about a hormonal environment that has shifted against you through a combination of changes that compound over time.
1. Declining estrogen and testosterone — in women, perimenopause and menopause bring a significant decline in estrogen, which shifts fat distribution toward the abdomen and reduces insulin sensitivity. In men, declining testosterone after 35–40 reduces lean muscle mass, which lowers the metabolic rate and reduces the body's capacity for glucose disposal. Both changes worsen the hormonal environment for fat burning.
2. Elevated baseline cortisol — chronic stress — which accumulates over decades of work, family, and financial pressure — produces chronically elevated cortisol that promotes visceral fat storage and directly worsens insulin resistance. By midlife, many people are carrying years of accumulated stress-driven hormonal dysfunction that no amount of dietary change alone can fully address.
3. Growth hormone decline — growth hormone peaks during adolescence and declines steadily through adulthood. By the time most people reach their 40s, growth hormone secretion is a fraction of its youthful levels — reducing the natural fat-burning and tissue-repair capacity that made staying lean effortless in earlier decades. The primary drivers of growth hormone release — deep sleep, fasting, and resistance exercise — are exactly what the MAP30 protocol is built around.
4. Compounding insulin resistance — insulin resistance typically develops over years and is rarely addressed until it crosses a diagnostic threshold. By 40, many people have a decade or more of accumulated insulin resistance that has progressively worsened the fat-storage environment. Addressing it at this stage requires more deliberate intervention — but the research is clear that it is fully reversible at any age with the right dietary approach.
If your weight gain accelerated after 40, it is not because your discipline suddenly failed. It is because the hormonal environment shifted against you. Understanding which specific shifts occurred is the first step to addressing them directly.
Is Your Weight Gain Hormones or Are You Overeating?
This is one of the most common questions in metabolic health — and the answer is almost always: both, but the hormones came first.
Here is the clinical reality: hormonal dysfunction drives overeating through specific mechanisms. Leptin resistance removes the satiety signal, so the brain never receives the message that fat stores are adequate. Ghrelin elevation after caloric restriction produces persistent hunger that overrides conscious restriction. Elevated insulin prevents the body from accessing stored fat, creating an energy deficit at the cellular level that drives hunger even when fat stores are abundant.
People who are overeating are often doing so because their hormonal system is sending a hunger signal that their body genuinely cannot ignore. Framing this as a willpower problem misses the mechanism entirely. The question is not whether they are overeating — it is why their hormonal system is driving them to overeat when they clearly have enough stored energy. Fix the hormonal environment and the overconsumption often resolves without requiring any active restriction.
"The body does not lie. If you are chronically hungry despite eating, something in the hormonal signaling is broken. Fix the hormones and the hunger resolves on its own."
How Intermittent Fasting Affects Your Hormones
When I first started intermittent fasting, I thought the benefit was purely caloric — a smaller eating window meant fewer opportunities to eat. What I discovered, and what the research consistently confirms, is that fasting produces measurable improvements across the full hormonal profile that operate entirely independently of caloric intake. This is one of the primary reasons it outperforms continuous caloric restriction for long-term metabolic health.
The hormonal chain that fasting activates runs in a specific sequence. Insulin falls first — the sustained low-insulin period that fasting creates is the prerequisite for everything that follows. Research consistently shows fasting insulin reductions of 20–31% within weeks of starting a regular fasting protocol. With insulin low, hormone-sensitive lipase activates and stored fat becomes available for energy — the fat-burning window that the eating pattern was keeping closed finally opens.
Growth hormone activates next, and the magnitude of its response to fasting is one of the most underappreciated findings in metabolic research. Studies show growth hormone increases of 1,300 to 2,000% during extended fasting periods — levels that promote fat mobilization, preserve lean muscle during the fasted state, and stimulate cellular repair. Unlike continuous caloric restriction, which suppresses growth hormone as the body interprets chronic energy deprivation as a threat, fasting triggers the growth hormone response precisely because the fasting signal is time-limited and the body reads it as a normal part of the daily rhythm.
After a five-day fast, mean 24-hour growth hormone secretion increased by more than 300% compared to the fed state, with the most dramatic increases occurring during the nocturnal secretory pulses. The study confirmed fasting as one of the most potent physiological stimulators of growth hormone — and established that even modest overnight fasting windows protect this pulse. (Ho KY et al. — Journal of Clinical Investigation, 1988)
Ghrelin and leptin follow a different but equally important pattern. Unlike continuous caloric restriction — which chronically elevates ghrelin and produces persistent hunger that erodes adherence — intermittent fasting adapts the ghrelin rhythm. After one to two weeks of consistent fasting, ghrelin pulses align with the eating window, making hunger predictable and manageable rather than constant. Leptin sensitivity gradually improves as visceral fat decreases and systemic inflammation falls. When implemented correctly — with adequate sleep and carbohydrate reduction — daily 12 to 16 hour fasting windows do not significantly elevate cortisol, which is the critical distinction between daily TRE and aggressive multi-day fasting.

How to Lose Fat Without Ruining Your Hormones
The most common way people damage their hormones while trying to lose fat is aggressive caloric restriction combined with excessive exercise. This combination produces the hormonal profile of starvation: elevated cortisol, elevated ghrelin, suppressed leptin, suppressed thyroid hormone, suppressed sex hormones, and reduced growth hormone. The body interprets extreme restriction as a threat to survival and adapts by slowing every system it can afford to slow.
The approach that improves body composition without hormonal disruption addresses fat loss through the hormonal environment rather than through energy deprivation. These are not six separate interventions — they are six inputs into the same hormonal system, and each one improves the environment in which the others operate:
Carbohydrate reduction — lowers insulin, the primary fat-storage hormone, without requiring caloric restriction — the fat-burning window opens when insulin falls, not when calories are cut
Daily fasting window of 12–16 hours — creates the sustained low-insulin period required for fat burning and triggers the growth hormone pulse that preserves lean mass during the fasted state
Adequate protein — preserves lean muscle mass through caloric deficits and suppresses ghrelin more effectively than carbohydrates or fat — each protein-forward meal is a satiety event
Zone 2 aerobic exercise — improves insulin sensitivity and fat oxidation without adding cortisol stress — the distinction between exercise that helps the hormonal environment and exercise that taxes it
7–9 hours of quality sleep — normalizes cortisol, ghrelin, leptin, and growth hormone simultaneously — the single highest-leverage intervention for the full hormonal profile
Stress management — reduces chronic cortisol elevation that drives visceral fat storage independent of diet — the hormonal damage from unmanaged stress cannot be outrun by dietary improvement alone
If you have been doing everything right and not seeing results, the answer is almost certainly in the hormonal environment. Understanding what these hormones are, what drives them, and what the research shows about improving them is the foundation everything else in the MAP30 framework is built on.
This article is part of our Hormones & Metabolism series. Hormones & Metabolism
Latest Articles

How to Burn Fat
You've been told your body runs on carbohydrates. That's only half the story. Understanding how ketones work in the body — and how to burn fat as fuel...

High Fructose Corn Syrup
The bigger question is not how many calories are in a soda. It is whether high fructose corn syrup is bad for you — and what repeated fructose exposure...

Fasting and Insulin Resistance
Your A1C came back normal. Your fasting glucose looks fine. Your doctor said everything is okay.

John Shaw
MAP30 Challenge
John Shaw is a Certified Nutrition Educator and the founder of the MAP30 Challenge. What began as a personal health journey at 294 pounds, and pre-diabetic, evolved into a structured 30-day metabolic reset program grounded in nutritional science. John's mission is simple: give people the biological education that the diet industry never did.
FAQ's
1. What are hormones and how do they work?
Hormones are chemical messengers produced by glands in the endocrine system that travel through the bloodstream and deliver instructions to cells and organs. They regulate metabolism, hunger, fat storage, energy production, sleep, stress response, and reproduction. Each hormone works by binding to a specific receptor on target cells — a lock-and-key mechanism that triggers a change in cellular behavior. The key metabolic hormones include insulin, glucagon, cortisol, leptin, ghrelin, growth hormone, and thyroid hormone.
2. What hormones block weight loss after 40?
Four hormonal shifts drive the weight gain many people experience after 40: declining estrogen in women, which shifts fat to the abdomen and reduces insulin sensitivity; declining testosterone in men and women, which reduces lean muscle mass and metabolic rate; elevated chronic cortisol from accumulated life stress, which promotes visceral fat storage; and progressive insulin resistance that has typically been developing for years before causing measurable blood sugar changes. Growth hormone also declines steadily after 30, reducing the body's natural fat-burning capacity.
3. Will hormones make me gain weight?
Hormonal imbalances are a primary driver of weight gain — particularly insulin resistance and the hormonal shifts associated with chronic stress and poor sleep. Elevated insulin prevents fat burning regardless of caloric intake. Elevated cortisol promotes visceral fat storage. Leptin resistance removes the satiety signal, driving hunger despite adequate fat stores. Ghrelin elevation after dieting produces persistent hunger that erodes adherence. In most cases of stubborn weight gain, the hormonal environment is the primary obstacle, not caloric intake.
4. How does intermittent fasting affect hormones?
Intermittent fasting improves the hormonal environment for fat burning through several mechanisms: it lowers fasting insulin by creating sustained low-insulin periods; it triggers significant growth hormone release of 1,300 to 2,000% during fasting; it adapts the ghrelin rhythm so hunger becomes predictable rather than constant; and it gradually improves leptin sensitivity as visceral fat decreases. Unlike continuous caloric restriction, which chronically elevates cortisol and ghrelin, intermittent fasting with adequate sleep does not trigger the hormonal stress response associated with starvation.
5. How do I know if my hormones are imbalanced?
Common signs of metabolic hormone imbalance include: stubborn weight gain especially around the abdomen despite dietary changes; fatigue not explained by sleep deprivation; persistent hunger and sugar cravings; difficulty losing weight on a calorie-restricted diet; poor sleep quality; mood instability; and elevated fasting glucose or fasting insulin on blood work. A fasting insulin test and HOMA-IR calculation can identify insulin resistance before A1C becomes abnormal. Thyroid, cortisol, and sex hormone panels can identify other contributors.
6. How do you optimize your hormones naturally?
The most evidence-supported natural interventions: consistent 7–9 hours of sleep, which normalizes cortisol, ghrelin, leptin, and growth hormone simultaneously; carbohydrate reduction and sugar elimination, which lowers insulin; a daily 12–16 hour fasting window, which promotes growth hormone release and insulin sensitivity; resistance exercise, which improves insulin sensitivity and supports testosterone; stress management, which reduces chronic cortisol elevation; and visceral fat reduction through the above interventions, which improves the overall hormonal environment.
Sources
Ebbeling CB et al. — 'Effects of dietary composition on energy expenditure during weight-loss maintenance' (JAMA, 2012) — https://pubmed.ncbi.nlm.nih.gov/22735432/
Ho KY et al. — 'Fasting enhances growth hormone secretion and amplifies the complex rhythms of growth hormone secretion in man' (Journal of Clinical Investigation, 1988) — https://pubmed.ncbi.nlm.nih.gov/3127426/
Reaven GM — 'Role of insulin resistance in human disease' (Diabetes, 1988) — https://pubmed.ncbi.nlm.nih.gov/3056758/
Leproult R & Van Cauter E — 'Role of sleep and sleep loss in hormonal release and metabolism' (Endocrine Development, 2010) — https://pubmed.ncbi.nlm.nih.gov/19955752/
Veldhuis JD et al. — 'Testosterone and estradiol regulate free insulin-like growth factor I' (JCEM, 1997) — https://pubmed.ncbi.nlm.nih.gov/9048572/
Epel ES et al. — 'Stress and body shape: stress-induced cortisol secretion is consistently greater among women with central fat' (Psychosomatic Medicine, 2000) — https://pubmed.ncbi.nlm.nih.gov/11020091/

Let Me See The Ai Audit Report
I had the MAP30 course material audited and graded by 4 dirrerent Ai models. I was shocked by the grade. See what they had to say about the MAP30 course.
Jaabsha Marketing LLC | All rights reserved 2024 Terms Of Service