6 April, 2026
Edition: Metabolic Disease
Vol 1, Edition 29
Non-Alcoholic Fatty Liver Disease: What Exactly Is NAFLD and Why Does It Happen?
You don't drink. You're not overweight. You eat reasonably well. And your doctor just told you that your liver is showing signs of fat accumulation. Here's what NAFLD actually is, why it has nothing to do with alcohol, and what's really causing it.
Published By: MAP30 Challenge | Authored By: John Shaw
Article Directory: https://map30challenge.com/article-directory
The NAFLD Progression Stages: Where Are You?
The NAFLD Progression Stages: Where Are You?
NAFLD moves in both directions — the same factors that drive progression also drive reversal when addressed
Simple Steatosis
Hepatic steatosis — fat accumulation without inflammation
Fat deposits in more than 5% of liver cells. No significant inflammation. Liver function largely intact. Most people at this stage have no symptoms — it's typically discovered on a routine ultrasound.
✅ Fully reversible with dietary intervention — typically within 8–12 weeks
NASH
Non-alcoholic steatohepatitis — fat with inflammation and cell damage
Fat accumulation plus active liver cell inflammation and damage. ALT and AST typically elevated. Liver under oxidative stress from lipid overload combined with inflammatory signaling from visceral fat and gut disruption.
⚠️ Reversible with sustained metabolic intervention — requires consistent dietary change over months
Fibrosis
Scar tissue replacing healthy liver tissue
The liver attempts to repair ongoing inflammatory damage by replacing damaged cells with scar tissue. Early fibrosis is partially reversible. Advanced fibrosis compromises liver function and is associated with significantly elevated cardiovascular risk independent of other metabolic factors.
🔴 Early stages partially reversible — progression can be halted and partially reversed with intervention
Cirrhosis
Extensive permanent scarring — liver architecture compromised
NAFLD-related cirrhosis is now the leading cause of liver transplant waitlisting in the United States, ahead of alcoholic liver disease. Liver architecture is permanently altered. Function is significantly impaired. Progression can be slowed but structural damage cannot be reversed.
🔴 Not reversible — medical management required. Progression can be slowed.
The ultrasound report uses careful language. "Hepatic steatosis." "Echogenic liver." "Consistent with fatty infiltration." Your doctor explains that there is fat accumulation in your liver — more than there should be. They may mention NAFLD. They may mention that it is "very common" and "usually nothing to worry about." They may suggest you lose some weight and come back in a year.
What they are less likely to explain is the mechanism behind it — how fat gets into a liver that has no business being fatty, what it means for the rest of your metabolic health, what happens if the process continues, and what actually reverses it. Those are the questions this article answers.
Because NAFLD is not a liver problem that happens to some unlucky people. It is a metabolic problem — one that sits directly downstream of insulin resistance, fructose overload, and the same dietary patterns that drive type 2 diabetes, visceral fat accumulation, and metabolic syndrome. The liver is where the consequences show up. The cause is in the food.
"Your liver didn't decide to fill itself with fat. It was instructed to. The instruction came from the food — specifically from fructose and chronically elevated insulin working together on a liver that had nowhere else to put the overflow."
What Exactly Is NAFLD?
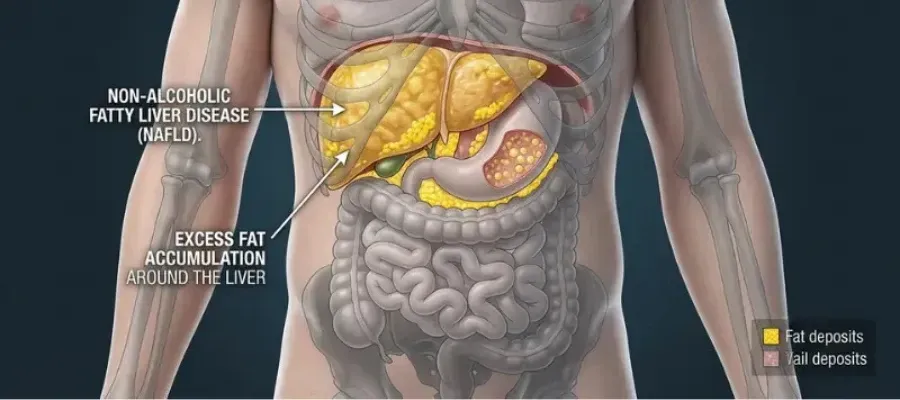
Non-alcoholic fatty liver disease is defined as fat accumulation in the liver — specifically, fat deposits comprising more than 5% of liver weight — in the absence of significant alcohol consumption and in the absence of other known causes of liver disease such as viral hepatitis or medication toxicity. The "non-alcoholic" in the name is important: NAFLD produces liver changes that are histologically identical to alcoholic liver disease, but without the alcohol.
It is now the most common chronic liver disease in the world. In the United States it affects an estimated 24 to 30% of the adult population — approximately 80 to 100 million people. Globally the estimate exceeds one billion. It is more prevalent than all forms of viral hepatitis combined, and its prevalence has been rising in direct proportion to the rise in obesity, type 2 diabetes, and metabolic syndrome over the past four decades.
NAFLD exists on a spectrum. At the mild end — simple steatosis, or hepatic steatosis — fat is present in liver cells but there is no significant inflammation and no liver cell damage. Many people at this stage have no symptoms and the condition is discovered incidentally on an ultrasound ordered for something else. At the severe end — non-alcoholic steatohepatitis (NASH), fibrosis, and cirrhosis — the liver is inflamed, scarred, and potentially failing. The progression from simple steatosis to NASH to cirrhosis is not inevitable, but it is also not rare. And it is entirely determined by whether the underlying metabolic drivers are addressed or not.
1 in 4 American adults
have NAFLD — most don't know it. It is now the leading cause of liver transplant waitlisting in the United States.
Younossi ZM et al. — Hepatology, 2016; AASLD Clinical Practice Guidelines, 2023
How Fat Gets Into the Liver — The Mechanism
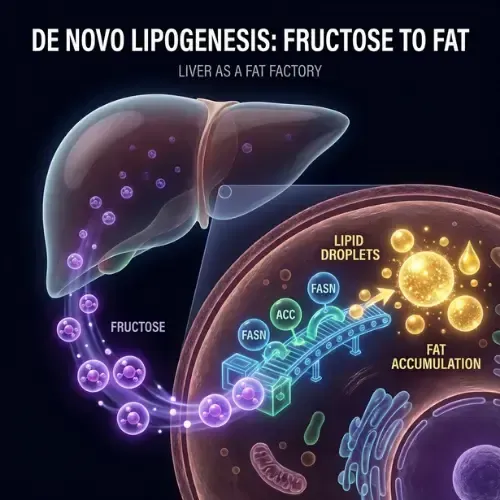
Understanding how NAFLD develops requires understanding de novo lipogenesis — the process by which the liver converts non-fat substrates, primarily carbohydrates and fructose, into fat. This is not a pathological process in itself. It is a normal hepatic function. The problem is when it is activated chronically and at high volume — which is exactly what happens in a diet high in refined carbohydrates, added sugars, and particularly fructose.
Fructose is the primary driver of hepatic fat accumulation. Unlike glucose — which can be used by virtually every cell in the body — fructose is metabolized almost exclusively in the liver. When fructose arrives at the liver in the quantities delivered by a diet high in added sugars and high-fructose corn syrup, the liver's processing capacity is overwhelmed. The excess fructose is converted directly to fat via de novo lipogenesis. That fat either enters the bloodstream as VLDL triglycerides or accumulates in liver cells themselves. Over time, with this pattern repeated daily, hepatic fat content rises.
Insulin resistance drives the second pathway. As covered in the Insulin Resistance article in this library, chronically elevated insulin promotes fat storage throughout the body — including in the liver. Insulin activates the enzyme fatty acid synthase in liver cells, promoting triglyceride synthesis. In a healthy liver with normal insulin sensitivity, this process is tightly regulated. In an insulin-resistant liver — which is almost always present alongside NAFLD — this regulation breaks down. The liver continues synthesizing fat even when fat stores are already elevated.
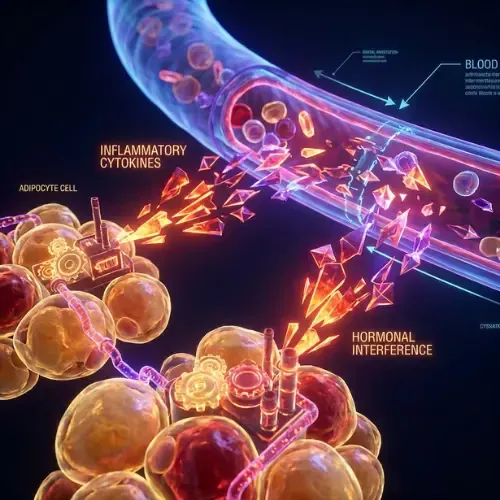
Visceral fat delivers a continuous inflammatory signal. Visceral adipose tissue drains directly into the portal vein — the blood vessel feeding the liver. As covered in the Visceral Fat article in this library, visceral fat continuously releases free fatty acids and pro-inflammatory cytokines including TNF-alpha and IL-6 directly into the portal circulation. The liver receives this inflammatory load first and in concentrated form. In people with significant visceral fat, the liver is being continuously exposed to both excess free fatty acids and inflammatory signaling that drives the progression from simple fat accumulation to inflammation and fibrosis.
Research by Samuel and Shulman at Yale demonstrated that hepatic insulin resistance — the liver's specific failure to respond normally to insulin's signal — is the central metabolic defect in NAFLD, and that it is driven by diacylglycerol accumulation in liver cells activating a kinase that blocks insulin receptor signaling. This establishes a direct mechanistic link between dietary fat and sugar overload, liver fat accumulation, and the insulin resistance that accelerates the disease. (Samuel VT, Shulman GI — Journal of Clinical Investigation, 2016)
Why NAFLD Affects Even Healthy Livers — And People Who Don't Drink
The most disorienting aspect of an NAFLD diagnosis for many people is that it doesn't fit their self-image. They don't drink heavily. They aren't significantly overweight. They may exercise regularly. And yet their liver shows fat accumulation that clinically resembles alcoholic liver disease.
The explanation is in the mechanism. NAFLD is not caused by alcohol. It is caused by fructose and insulin-driven de novo lipogenesis — a process that alcohol happens to also activate, which is why the end result looks the same. A person who drinks no alcohol but consumes significant amounts of added sugar, refined carbohydrates, and high-fructose corn syrup is subjecting their liver to the same metabolic load as a moderate drinker. The substrate is different. The hepatic outcome is similar.
The liver doesn't ask where the fructose came from. It processes what it receives through the portal vein — and the portal vein delivers everything from the gut. This is why the NAFLD risk profile is broader than most people realize. Insulin resistance is present in an estimated 70 to 80 percent of NAFLD patients regardless of body weight. Type 2 diabetes is accompanied by NAFLD in approximately 70 percent of cases. Metabolic syndrome — even one or two components — significantly elevates risk. Gut microbiome disruption increases intestinal permeability, flooding the portal circulation with bacterial endotoxins that drive hepatic inflammation. And paradoxically, rapid weight loss can worsen NAFLD temporarily by mobilizing large volumes of fat into the portal circulation faster than the liver can process it.

This also explains lean NAFLD — a condition increasingly documented in people with normal BMI who carry significant visceral fat and hepatic fat accumulation. Their total body weight looks normal. What the scale doesn't show is where the fat is deposited, or what the liver has been receiving through the portal vein for years. The liver responds to what it's sent. It doesn't negotiate with the number on the scale.
"The liver processes everything that comes through the portal vein. Every gram of fructose, every surge of insulin, every free fatty acid from visceral fat — it all arrives at the liver first. NAFLD is what happens when the liver runs that gauntlet for years without a break."
The Four Stages of NAFLD — And What Determines Progression
NAFLD is not a single condition. It is a spectrum — and where a person sits on that spectrum, and whether they progress, is almost entirely determined by the metabolic environment their liver is operating in.
Simple steatosis — Stage 1 — is fat accumulation in liver cells without inflammation. The liver is enlarged and echogenic on ultrasound but liver cell function is largely intact. At this stage, the condition is fully reversible with metabolic intervention. Most people at Stage 1 have no symptoms.
Non-alcoholic steatohepatitis (NASH) — Stage 2 — is fat accumulation with liver cell inflammation and damage. This is the inflection point. Liver enzymes — ALT and AST — are typically elevated. The liver is under active oxidative stress from the combination of lipid overload and inflammatory signaling. At this stage, reversal is still achievable but requires more sustained intervention. Left unaddressed, NASH progresses.
Fibrosis — Stage 3 — is the replacement of healthy liver tissue with scar tissue as the liver attempts to repair the ongoing inflammatory damage. Early fibrosis is reversible. Advanced fibrosis begins to compromise liver function and is only partially reversible. This is the stage at which NAFLD begins to have systemic consequences beyond metabolic health — including elevated cardiovascular risk independent of other factors.
Cirrhosis — Stage 4 — is extensive scarring that permanently impairs liver architecture and function. At this stage the liver cannot regenerate. Cirrhosis from NAFLD is now the leading cause of liver transplant waitlisting in the United States, having overtaken alcoholic liver disease and viral hepatitis. It is not reversible, but its progression can be slowed.
A 20-year prospective study found that approximately 20% of people with NASH progressed to cirrhosis over that period, while those with simple steatosis showed a much lower progression rate. The strongest predictor of progression was not the degree of initial fat accumulation but the presence and severity of insulin resistance and metabolic syndrome components. (Ekstedt M et al. — Hepatology, 2015)
The most important clinical point from the progression research is this: the stage of NAFLD is not fixed. It moves — in both directions. The same dietary and lifestyle factors that drive progression also, when removed, drive regression. Stage 1 and Stage 2 NAFLD are reversible. The window is open.
Can NAFLD Be Reversed — And What the Evidence Actually Shows
There is currently no FDA-approved medication for NAFLD. The entire evidence base for reversal is dietary and lifestyle intervention — which means the same metabolic conditions that caused the problem are the levers for reversing it.
The foundation is removing the primary input driving hepatic fat synthesis in the first place. Fructose from added sugars and high-fructose corn syrup is the liver's most direct fat-production instruction. Clinical trials consistently show measurable reductions in liver fat content within eight to twelve weeks of fructose elimination, independent of total caloric change. Not reduced. Eliminated from daily intake. The liver cannot produce less fat if it keeps receiving the signal to produce more.
From that foundation, reducing refined carbohydrates addresses the second pathway — the chronic insulin elevation that activates hepatic fatty acid synthase and keeps the liver in fat-producing mode. Low-carbohydrate interventions consistently produce greater liver fat reduction than low-fat calorie-restricted diets at equivalent weight loss, because they address the insulin signal directly rather than just the caloric load. Fasting windows then create the daily low-insulin periods where the liver can begin oxidizing the fat it has already accumulated. The liver burns fat during the fasted state just as adipose tissue does — but only when insulin falls far enough to allow it. Regular 12 to 14-hour overnight fasting windows create that metabolic space every day.
Visceral fat reduction closes the loop from the other direction. Because visceral fat continuously delivers free fatty acids and inflammatory signals directly to the liver via the portal vein, reducing it simultaneously reduces both the fat load and the inflammatory burden driving progression from steatosis toward NASH and fibrosis. The interventions that most efficiently reduce visceral fat — carbohydrate restriction and fasting — are the same ones that reduce liver fat. They operate through overlapping mechanisms, which is why their combined effect is greater than either alone.

The gut-liver axis is the final piece most people don't connect to liver health. Gut microbiome disruption increases intestinal permeability, allowing bacterial lipopolysaccharides to enter the portal circulation and reach the liver, driving the inflammatory progression that separates simple steatosis from NASH. Dietary fiber diversity, fermented foods, and elimination of the emulsifiers in ultra-processed foods that degrade the gut barrier all reduce this hepatic inflammatory load through a pathway that has nothing directly to do with calories or carbohydrates.
The liver is one of the most metabolically responsive organs in the body. In patients with Stage 1 and Stage 2 NAFLD, meaningful liver fat reduction appears within eight to twelve weeks of consistent dietary change — measurable on follow-up ultrasound and in liver enzyme normalization. The window is open longer than most people realize. The stage is not a sentence. It is a description of where things stand right now — and it moves in both directions.
This article is part of our Metabolic Disease series. Metabolic Disease
Latest Articles
Glucagon Benefits for Fat Loss
Every conversation about blood sugar and fat loss focuses on insulin. But insulin has a counterpart that does the opposite job — and understanding it may be more important.
Visceral Fat vs. Subcutaneous Fat
Not all body fat is equal — and the difference matters more than almost anything else in metabolic health. One type stores energy quietly.
Improve Metabolic Flexibility
Metabolic flexibility is the ability to switch efficiently between burning glucose and burning fat depending on what fuel is available. Most people have lost it.

John Shaw
MAP30 Challenge
John Shaw is a Certified Nutrition Educator and the founder of the MAP30 Challenge. What began as a personal health journey at 294 pounds, and pre-diabetic, evolved into a structured 30-day metabolic reset program grounded in nutritional science. John's mission is simple: give people the biological education that the diet industry never did.
FAQ's
1. What exactly is NAFLD?
Non-alcoholic fatty liver disease is fat accumulation in the liver — more than 5% of liver weight — in the absence of significant alcohol consumption. It is the most common chronic liver disease in the world, affecting approximately 1 in 4 American adults. It exists on a spectrum from simple steatosis — fat without inflammation, fully reversible — through NASH, fibrosis, and cirrhosis. The underlying cause is not alcohol but fructose-driven de novo lipogenesis and insulin resistance-driven hepatic fat synthesis.
2. Why does NAFLD affect people who don't drink?
Because NAFLD is not caused by alcohol. It is caused by fructose and insulin-driven de novo lipogenesis — the same process alcohol activates, which is why the liver changes look identical. A person who consumes significant added sugars and refined carbohydrates without drinking is subjecting their liver to an equivalent metabolic load through a different substrate. The liver responds to the fructose and insulin signals it receives — not to whether alcohol is present.
3. Can NAFLD be reversed?
Yes — Stages 1 and 2 are fully reversible with dietary and lifestyle intervention. There is no FDA-approved medication for NAFLD; the entire evidence base is dietary. Eliminating fructose and added sugar, reducing refined carbohydrates, incorporating fasting windows, reducing visceral fat, and supporting gut barrier integrity all produce measurable liver fat reduction. Clinical trials show significant improvements within eight to twelve weeks of consistent intervention.
4. What foods cause fatty liver disease?
The primary dietary drivers are fructose from added sugars and high-fructose corn syrup, which the liver converts directly to fat via de novo lipogenesis; refined carbohydrates that drive chronic insulin elevation and hepatic fat synthesis; and ultra-processed foods whose emulsifiers disrupt gut barrier integrity and increase the bacterial endotoxin load delivered to the liver via the portal vein. Alcohol is a separate pathway producing the same outcome through a different mechanism.
5. What are the stages of NAFLD?
Four stages: simple steatosis — fat without inflammation, fully reversible; NASH — fat with inflammation and liver cell damage, reversible with sustained intervention; fibrosis — scar tissue replacing healthy liver tissue, early stages partially reversible; and cirrhosis — extensive permanent scarring, not reversible. Progression between stages is driven by the persistence and severity of the underlying metabolic drivers — particularly insulin resistance and visceral fat.
6. Does NAFLD cause symptoms?
In early stages — simple steatosis and even early NASH — NAFLD typically produces no symptoms. Most cases are discovered incidentally on ultrasound ordered for another reason, or through persistently elevated ALT on a routine blood panel. As the disease progresses to advanced fibrosis and cirrhosis, symptoms including fatigue, right upper quadrant discomfort, and signs of liver dysfunction may appear. The absence of symptoms in early NAFLD is one of the primary reasons it goes undetected until it has already progressed.
Sources
Younossi ZM et al. — 'Global epidemiology of nonalcoholic fatty liver disease' (Hepatology, 2016) — https://pubmed.ncbi.nlm.nih.gov/26707365/
Samuel VT, Shulman GI — 'Mechanisms for insulin resistance: common threads and missing links' (Cell, 2012) — https://pubmed.ncbi.nlm.nih.gov/22424228/
Ekstedt M et al. — 'Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD' (Hepatology, 2015) — https://pubmed.ncbi.nlm.nih.gov/25125077/
Lustig RH — 'Fructose: It's Alcohol Without the Buzz' (Advances in Nutrition, 2013) — https://pubmed.ncbi.nlm.nih.gov/23408191/
Chalasani N et al. — 'The diagnosis and management of nonalcoholic fatty liver disease' (Hepatology, 2018) — https://pubmed.ncbi.nlm.nih.gov/29152943/
Cani PD et al. — 'Metabolic Endotoxemia Initiates Obesity and Insulin Resistance' (Diabetes, 2007) — https://pubmed.ncbi.nlm.nih.gov/17519319/

Let Me See The Ai Audit Report
I had the MAP30 course material audited and graded by 4 dirrerent Ai models. I was shocked by the grade. See what they had to say about the MAP30 course.
Jaabsha Marketing LLC | All rights reserved 2024 Terms Of Service