Edition: Weight Loss & Fat Burning
2 April, 2026
In The News
Vol 1, Edition 26
Visceral Fat vs. Subcutaneous Fat: Which One Is Actually Dangerous?
Not all body fat is equal — and the difference matters more than almost anything else in metabolic health. One type stores energy quietly. The other secretes hormones, drives inflammation, and actively dismantles your insulin signaling. Understanding which is which changes everything about how you approach fat loss.
Published By: MAP30 Challenge
Authored By: John Shaw
Visceral Fat vs. Subcutaneous Fat: What Makes Them Different
Visceral Fat vs. Subcutaneous Fat: What Makes Them Different
🟢 Subcutaneous Fat
Under the skin · Visible · Pinchable
Location
Between skin and muscle — abdomen, hips, thighs, arms. Visible in the mirror.
Drainage pathway
Drains into systemic circulation — inflammatory output diluted across the whole body.
Metabolic activity
Lower lipolytic rate. Relatively passive energy storage. Less hormonally active.
Inflammatory output
Modest cytokine secretion, diluted into systemic circulation. Not independently linked to metabolic disease at moderate levels.
Metabolic risk
Low to moderate at typical levels. Gluteofemoral fat in women may even be metabolically protective.
🔴 Visceral Fat
Around organs · Invisible · Metabolically active
Location
Inside the abdominal cavity, surrounding the liver, pancreas, kidneys, and intestines. Cannot be seen or pinched.
Drainage pathway
Drains directly into the portal vein — inflammatory molecules hit the liver first, in concentrated form.
Metabolic activity
High lipolytic rate. Highly responsive to cortisol and catecholamines. Behaves like an active endocrine organ.
Inflammatory output
Continuously secretes TNF-alpha, IL-6, and resistin into portal circulation. Suppresses adiponectin. Drives hepatic insulin resistance.
Metabolic risk
High at any significant level. Independently associated with insulin resistance, metabolic syndrome, type 2 diabetes, and cardiovascular disease.
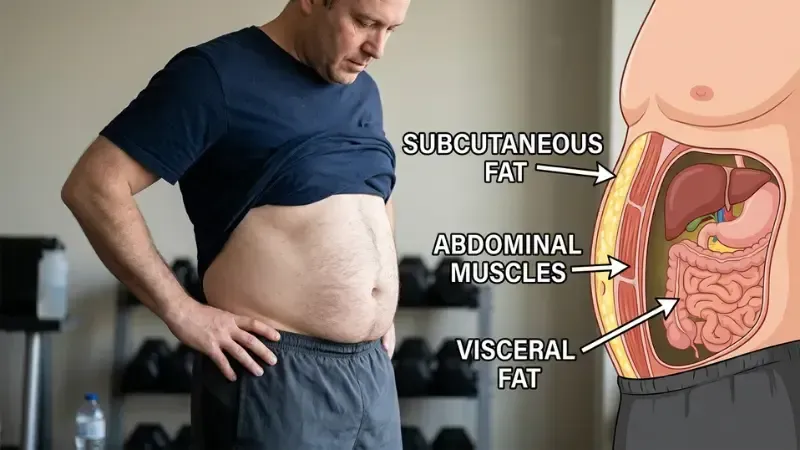
Stand in front of a mirror and pinch the fat on your waist. That's subcutaneous fat — the layer sitting between your skin and muscle. It's visible, it's pinchable, and for most of your life it's been the fat you've been trying to lose. It is largely benign.
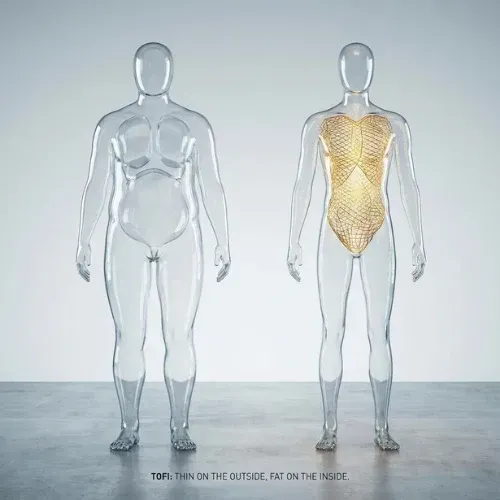
Now think about the fat you can't see or pinch — the fat packed around your liver, your pancreas, your intestines, and your heart. That's visceral fat. You can't feel it. A person can have a relatively flat stomach and dangerous levels of visceral fat deposited around their organs. It is not measured by how you look. It is measured by metabolic consequence.
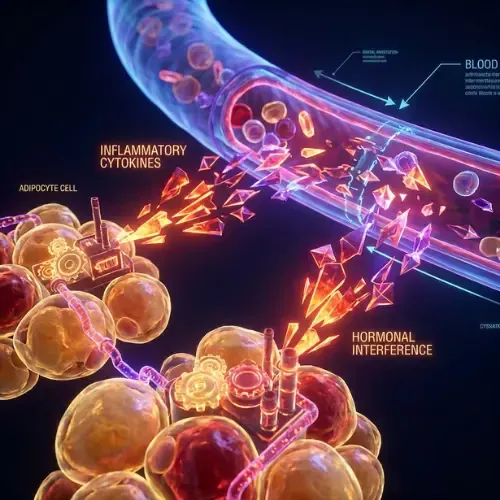
These two types of fat are chemically different, metabolically different, and hormonally different. Subcutaneous fat behaves largely like a passive energy reserve. Visceral fat behaves like an endocrine organ — one that is continuously secreting pro-inflammatory cytokines, disrupting insulin signaling, and driving the hormonal cascade that produces metabolic syndrome, type 2 diabetes, and cardiovascular disease.
The scale doesn't distinguish between them. BMI doesn't distinguish between them. Understanding the difference is not academic — it determines what you should actually be targeting and why.
Visceral Fat vs Subcutaneous Fat — What Makes Them Different
What I want you to understand is that distinction starts with location. Subcutaneous fat lies just beneath the skin and above the muscle — spread across the abdomen, thighs, hips, and arms. It is the fat visible in the mirror, the fat that changes clothing sizes, the fat that responds to exercise in the way most people expect.
Visceral fat lies inside the peritoneal cavity, wrapping around the liver, pancreas, kidneys, and intestines. Its anatomical position is its defining danger: visceral fat drains directly into the portal vein — the blood vessel that feeds the liver. Every inflammatory molecule and free fatty acid released by visceral fat reaches the liver first, in concentrated form, before entering the rest of the body. Subcutaneous fat has no equivalent pathway.
Visceral fat cells have significantly higher rates of lipolysis, higher inflammatory cytokine secretion, and greater sensitivity to stress hormones including cortisol and catecholamines than subcutaneous fat cells of the same mass. (Frayn KN, Karpe F — International Journal of Obesity, 2014)
The metabolic consequences follow directly from this biology. Visceral fat continuously secretes TNF-alpha, IL-6, and resistin into the portal circulation — driving hepatic insulin resistance, promoting non-alcoholic fatty liver disease, and suppressing adiponectin. Subcutaneous fat, releasing the same molecules into the dilute systemic circulation, produces a fraction of the same disruption at equivalent volumes.
The practical implication is that two people with identical body weight can have dramatically different metabolic health profiles depending on where their fat is distributed. The person carrying more visceral fat and less subcutaneous fat has higher inflammatory burden, worse insulin sensitivity, higher cardiovascular risk, and greater likelihood of metabolic syndrome — regardless of what the scale says.
Why Visceral Fat Accumulates — The Cortisol and Insulin Connection
Visceral fat is not simply the result of eating too much. It is the result of a specific hormonal environment — one driven by chronically elevated cortisol, insulin resistance, and the body's fat distribution being pushed toward abdominal deposition.
Visceral adipose tissue has a higher density of glucocorticoid receptors than subcutaneous fat, making it more responsive to cortisol. Chronic stress, poor sleep, and HPA axis dysregulation produce sustained cortisol elevation that preferentially drives fat storage in the visceral compartment. This is why the relationship between stress and belly fat gain is not metaphorical. It is receptor-mediated and mechanistically documented.
Insulin resistance compounds this. Chronically elevated insulin keeps fat cells in storage mode — and visceral fat cells, with their high metabolic activity, are particularly sensitive to this signal. The fat accumulates readily and is difficult to deplete when both insulin and cortisol are simultaneously elevated. Both hormones have to shift for visceral fat to meaningfully recede.
Men and postmenopausal women disproportionately accumulate visceral fat compared to premenopausal women — a difference mediated by estrogen's protective effect on fat distribution. The loss of estrogen at menopause shifts fat storage preferentially to the visceral compartment. (Karastergiou K et al. — Biology of Sex Differences, 2012)

"Visceral fat is not a storage problem. It is a hormonal problem. Fix the hormonal environment and visceral fat recedes. Chase the scale without fixing the hormones and it stays."
How to Tell If You Have Too Much Visceral Fat
MRI and CT scan are the gold standard for measuring visceral fat volume — neither is practical for routine monitoring. The most reliable accessible proxies are waist circumference, waist-to-height ratio, and a panel of metabolic blood markers.
If you meet three or more of these criteria simultaneously, visceral fat is likely driving metabolic syndrome:
Waist circumference above 35 inches (women) or 40 inches (men)
Fasting triglycerides above 150 mg/dL
HDL cholesterol below 50 mg/dL (women) or 40 mg/dL (men)
Fasting insulin above 10 μIU/mL — or HOMA-IR above 2.0
Elevated hsCRP — the chronic low-grade inflammation marker
Waist circumference above 35 inches (89 cm) in women and 40 inches (102 cm) in men correlates strongly with elevated visceral fat and increased metabolic risk across most population studies. Waist-to-height ratio — waist divided by height — performs slightly better and has the advantage of being consistent across different body sizes and ethnic populations. DEXA scan, increasingly available through sports medicine and body composition clinics, provides the most accessible high-accuracy measurement outside of imaging.
What Happens When Visceral Fat Finally Starts to Break Down
Visceral fat responds to metabolic intervention faster than subcutaneous fat — its higher metabolic activity means it mobilizes more readily when the right hormonal conditions are established. And when it starts to go, the downstream effects are immediate and measurable.
Fasting insulin begins to fall within weeks of meaningful carbohydrate reduction. Systemic inflammation decreases as cytokine secretion from the visceral compartment drops. Liver fat reduces as portal free fatty acid delivery normalizes. Triglycerides fall. HDL rises. Waist circumference decreases before body weight changes significantly — because visceral fat is more metabolically active and mobilizes faster than subcutaneous fat. Most people notice improved energy and reduced cravings before the scale moves meaningfully.
Four interventions have the most consistent evidence for producing this result:
Reducing dietary refined carbohydrates and added sugars produces the most reliable visceral fat reduction of any dietary approach. Visceral fat accumulation is driven primarily by elevated insulin and fructose-driven hepatic lipogenesis. Lowering carbohydrate intake addresses both simultaneously. Multiple controlled trials comparing low-carbohydrate to low-fat diets at equivalent calories consistently show greater visceral fat loss — not just total fat loss — in the low-carbohydrate group.
Sleep quality has a direct and dose-dependent relationship with visceral fat accumulation. Even modest sleep restriction — six hours instead of eight over two weeks — produces measurable cortisol increases and visceral fat deposition independent of caloric intake. Sleep is one of the fastest-acting and most overlooked levers for both accumulating and removing visceral fat.
Sleep quality has a direct and dose-dependent relationship with visceral fat accumulation. Even modest sleep restriction — six hours instead of eight over two weeks — produces measurable cortisol increases and visceral fat deposition independent of caloric intake. Sleep is one of the fastest-acting and most overlooked levers for both accumulating and removing visceral fat.
Resistance exercise reduces visceral fat through skeletal muscle insulin sensitization. Consistent resistance training two to three times per week produces measurable visceral fat reduction within eight weeks — primarily by improving skeletal muscle glucose disposal, which lowers fasting insulin over time and removes one of the primary hormonal drivers of visceral deposition.
The most meaningful progress marker throughout is not the scale — it is waist circumference, measured weekly at the same time and conditions. Waist circumference reflects visceral fat change directly. It is the number that tells you whether the metabolic environment is actually shifting, not just whether total body mass is decreasing.
Key Takeaways
Visceral fat and subcutaneous fat are chemically, metabolically, and hormonally different — they are not the same fat in different locations
Visceral fat is dangerous because it drains directly into the portal vein, concentrating inflammatory molecules at the liver and driving insulin resistance, fatty liver, and metabolic syndrome
You can have dangerous visceral fat with a normal BMI and a relatively flat stomach — the scale and the mirror don't measure it
Visceral fat is primarily a hormonal problem driven by chronically elevated insulin and cortisol — not a simple calorie excess
The most effective interventions target the hormonal environment directly: reduce refined carbohydrates, extend fasting windows, improve sleep, add resistance exercise
Track waist circumference, not body weight — it is the most accessible daily proxy for visceral fat change
This article is part of our Weight Loss & Fat Burning series. Weight Loss & Fat Burning
Latest Articles

24-Hour Fasting Benefits
A 16-hour fast and a 24-hour fast are not just different in duration — they produce different metabolic events. Here's what changes in that second half of the day.
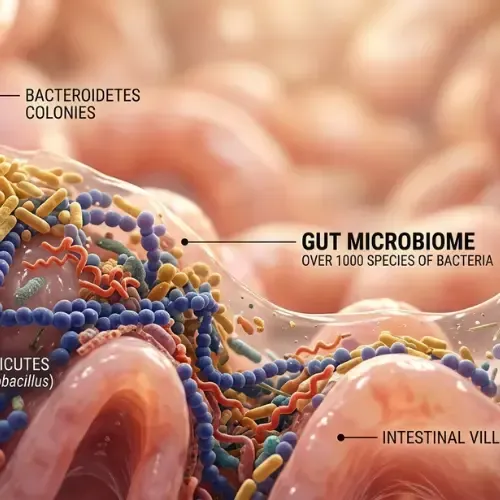
Improve Your Gut Microbiome
You have more bacterial cells in your gut than human cells in your entire body. Most people know the gut microbiome exists. Almost nobody understands what it actually does

What Is HOMA-IR
Most people with insulin resistance have normal blood sugar. That's exactly why the standard blood sugar test misses it. HOMA-IR — a calculation using fasting insulin and fasting glucose

John Shaw
MAP30 Challenge
John Shaw is a Certified Nutrition Educator and the founder of the MAP30 Challenge. What began as a personal health journey at 294 pounds, and pre-diabetic, evolved into a structured 30-day metabolic reset program grounded in nutritional science. John's mission is simple: give people the biological education that the diet industry never did.
FAQ's
1. What is the difference between visceral fat and subcutaneous fat?
Subcutaneous fat sits between skin and muscle — visible, pinchable, and largely a passive energy reserve. Visceral fat surrounds internal organs within the abdominal cavity and drains directly into the portal circulation feeding the liver. It is metabolically active, secreting inflammatory cytokines and free fatty acids that drive insulin resistance, chronic inflammation, and metabolic disease. Subcutaneous fat at moderate levels is largely benign. Visceral fat at any significant level is not.
2. Why is visceral fat more dangerous than subcutaneous fat?
Visceral fat cells have higher metabolic activity, higher inflammatory cytokine secretion, and higher sensitivity to stress hormones than subcutaneous fat cells. Their venous drainage empties directly into the portal vein, concentrating inflammatory molecules at the liver before systemic circulation. This produces hepatic insulin resistance, promotes fatty liver disease, suppresses adiponectin, and drives metabolic syndrome. Subcutaneous fat does not share this anatomical pathway.
3. How do you know if you have too much visceral fat?
Practical indicators: waist circumference above 35 inches (women) or 40 inches (men); fasting triglycerides above 150 mg/dL; HDL below 50 mg/dL (women) or 40 mg/dL (men); HOMA-IR above 2.0; and elevated hsCRP. Three or more simultaneously indicates metabolic syndrome, of which high visceral fat is almost always the driver. DEXA scan provides the most accessible accurate measurement. Waist-to-height ratio is the best single daily proxy.
4. What causes visceral fat to accumulate?
A specific hormonal environment: chronically elevated insulin driving fat storage; elevated cortisol from chronic stress and poor sleep activating visceral adipose tissue's high-density glucocorticoid receptors; and fructose-driven hepatic lipogenesis from high refined carbohydrate intake. Visceral fat is primarily a hormonal problem, not a caloric one. Normal-weight people with chronically elevated cortisol and insulin can accumulate significant visceral fat while maintaining a flat external appearance.
5. What happens when visceral fat finally starts to break down?
As visceral fat mobilizes, fasting insulin falls — often measurably within weeks. Systemic inflammation decreases as cytokine secretion from the visceral compartment drops. Liver fat reduces as portal free fatty acid delivery normalizes. Triglycerides fall. HDL rises. Waist circumference decreases before body weight changes significantly. Most people notice improved energy and reduced cravings before the scale moves meaningfully.
6. Can you have visceral fat without being overweight?
Yes — and this is one of the most clinically important facts about visceral fat. Normal-weight individuals with high visceral fat have equivalent cardiovascular and metabolic risk to obese individuals. A person can have a normal BMI, a relatively flat stomach, and dangerous visceral fat levels around their organs. The only reliable ways to identify it are waist circumference measurement, DEXA scan, or metabolic blood markers including fasting insulin and triglycerides.
Sources
Després JP et al. — 'Abdominal obesity and metabolic syndrome' (Nature, 2006) — https://pubmed.ncbi.nlm.nih.gov/17122770/
Frayn KN, Karpe F — 'Substrate utilization in human adipose tissues' (International Journal of Obesity, 2014) — https://pubmed.ncbi.nlm.nih.gov/23736370/
Karastergiou K et al. — 'Sex differences in human adipose tissues' (Biology of Sex Differences, 2012) — https://pubmed.ncbi.nlm.nih.gov/22651247/
Goss AM et al. — 'Effects of diet macronutrient composition on body composition' (Obesity, 2013) — https://pubmed.ncbi.nlm.nih.gov/22960796/
Spiegel K et al. — 'Sleep loss: a novel risk factor for insulin resistance' (Journal of Applied Physiology, 2005) — https://pubmed.ncbi.nlm.nih.gov/16227462/

Let Me See The Ai Audit Report
I had the MAP30 course material audited and graded by 4 dirrerent Ai models. I was shocked by the grade. See what they had to say about the MAP30 course.
Jaabsha Marketing LLC | All rights reserved 2024 Terms Of Service