10 April, 2026
Edition: Fasting & Metabolic Reset
Vol 1, Edition 26
Can Intermittent Fasting Help With Insulin Resistance? Here's What the Science Shows
Intermittent fasting is the most talked-about dietary intervention of the past decade. But most of the conversation focuses on weight loss. The more important question — and the one with the most compelling science behind it — is what fasting does to insulin resistance. Here's the mechanism, what the research shows, and how to use it.
Published By: MAP30 Challenge | Authored By: John Shaw
Article Directory: https://map30challenge.com/article-directory
Here is a question most intermittent fasting articles never ask: why does it work?
Not the weight loss — that part is explained easily enough by reduced eating windows and fewer opportunities to consume calories. The more interesting question is why intermittent fasting consistently improves metabolic markers — fasting insulin, HOMA-IR, triglycerides, blood pressure — in a way that calorie restriction alone does not reliably produce, even when the total calories consumed are identical.
The answer is not calories. It is time. Specifically, it is the duration during which insulin is low enough for specific biological processes to activate — processes that calorie restriction without a genuine fasting window does not trigger with the same consistency. Understanding this distinction explains what intermittent fasting actually does to insulin resistance, and it explains what is happening in your body during every hour you are not eating.
"Intermittent fasting is not a calorie restriction strategy that happens to involve skipping meals. It is a hormonal intervention that happens to reduce calorie intake. The mechanism is insulin. The meal timing is just how you activate it."
What Intermittent Fasting Actually Is
Intermittent fasting is not a diet in the conventional sense. It does not specify what you eat. It specifies when. The core principle is an eating window and a fasting window. The most widely studied protocol is the 16:8 — sixteen hours of fasting, eight hours of eating. Other protocols include the 18:6, the 20:4, and alternate day fasting. All operate through the same fundamental mechanism at different intensities.
The confusion about IF comes from the weight loss framing. When evaluated as a weight loss tool against calorie restriction, controlled studies where calories are matched show similar total weight loss. That comparison misses the point. Where IF's value lies is in the metabolic effects the fasting window produces that continuous calorie restriction does not consistently replicate — greater improvements in fasting insulin, HOMA-IR, triglycerides, and inflammatory markers, driven by the hours of low insulin the eating restriction creates rather than the caloric deficit alone.
The Insulin Mechanism — Why the Fasting Window Changes Everything
Every hour after your last meal is an hour of falling insulin. This is simple physiology — insulin rises in response to food, particularly carbohydrates, and falls when food stops. The question is how low it falls, and for how long, before the next meal interrupts the process.
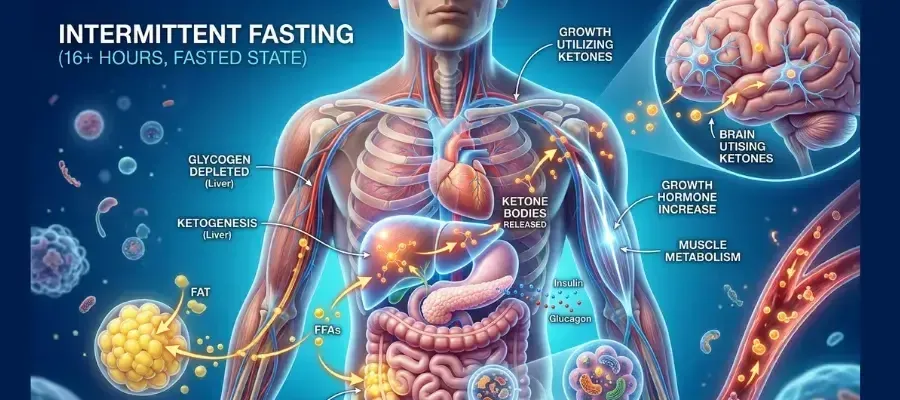
The 16:8 Fasting Window: What's Happening Hormonally Hour by Hour
The 16:8 Fasting Window: What's Happening Hormonally Hour by Hour
7pm — Last meal
Eating window closes
Insulin rises with the meal, then begins falling. The fasting clock starts here.
7pm–11pm (Hours 0–4)
Insulin falling
Blood glucose normalizing. Liver processing meal nutrients. Minimal fat burning.
11pm–7am (Hours 4–12)
Glycogen depleting
Insulin continues falling. Liver begins drawing on glycogen. Fat burning increasing. Growth hormone rising during deep sleep.
7am–9am (Hours 12–14)
🔄 The metabolic switch
Liver glycogen largely depleted. Glucagon elevated. HSL active — stored fatty acids releasing. Ketone production begins. This is the threshold for meaningful metabolic benefit.
9am–11am (Hours 14–16)
🔥 Peak fasting state
Fat oxidation well-established. Insulin at nadir. Autophagy significantly upregulated. Insulin sensitivity actively recovering. This is where 16:8 delivers its greatest daily metabolic value.
11am — First meal
Eating window opens
Break the fast with protein and healthy fats. The metabolic work of the fasting window is done. Repeat tomorrow.
In a continuous eating pattern, insulin never reaches its nadir. Three meals plus snacks spaced throughout the day means insulin rises after each eating event and begins falling during the gap — but another meal arrives before it reaches the low baseline required for fat burning and insulin sensitivity recovery to fully activate. The system is never given the sustained low-insulin window that allows these processes to run to completion.
In a 16:8 fasting protocol, the overnight fast extends from dinner until the first meal the following day. If dinner ends at 7pm and the first meal is at 11am, insulin has been falling for 16 hours. By hours 12 to 14, liver glycogen is depleted. Glucagon rises. The metabolic switch activates. Fat oxidation becomes the primary fuel source. By hour 16, insulin has reached its genuine nadir, autophagy is significantly upregulated, and the hormonal conditions for insulin sensitivity recovery are fully established.
For people with insulin resistance, the nadir takes longer to reach because fasting insulin is chronically elevated. The first weeks of fasting may produce less dramatic results because insulin never falls far enough. This is why dietary composition change — particularly reducing refined carbohydrates — works synergistically with fasting: lower carbohydrate intake means lower insulin peaks after meals, which means insulin falls further and faster during the fasting window, amplifying every hour of the fast.
A randomized controlled trial in men with prediabetes found that early time-restricted feeding — eating within a 6-hour window in the morning — significantly improved insulin sensitivity, blood pressure, and oxidative stress compared to controls eating the same foods across a 12-hour window, without any difference in caloric intake or weight loss. The improvements were attributed entirely to the extended fasting period. (Sutton EF et al. — Cell Metabolism, 2018)
What Happens to Your Body During a Fast — The Hourly Sequence
The metabolic changes during a fasting window unfold in a specific sequence. Each stage builds on the previous one — which is why extending the fast beyond 12 hours produces meaningfully different effects than stopping at 10.
Hours 0–4: Blood glucose and insulin are falling from the postprandial peak. The body is still processing and storing nutrients from the last meal. Fat burning is minimal.
Hours 4–8: Insulin has fallen substantially. Glucagon begins rising. The liver draws on glycogen stores to maintain blood glucose. Fat burning begins activating at the margins.
Hours 8–12: Liver glycogen is being actively depleted. The shift from glucose oxidation toward fat oxidation is underway. This is where a typical overnight fast — dinner at 7pm, breakfast at 7am — sits. Adequate, but not the full benefit.
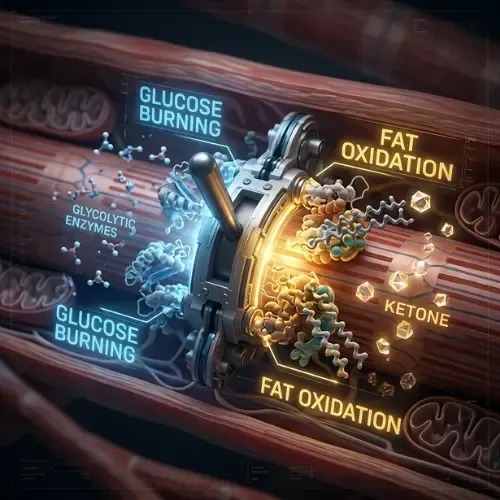
Hours 12–14: The metabolic switch point. Liver glycogen is largely depleted. Hormone-sensitive lipase is active. Fatty acids are being released from adipose tissue and converted to ketones. This is the threshold most fasting research identifies for meaningful metabolic benefit.
Hours 14–16: Fat oxidation is well-established. Insulin has reached its nadir. Growth hormone — which supports fat mobilization and lean mass preservation — begins rising. Autophagy is significantly upregulated. This is where the 16:8 protocol delivers its greatest metabolic value per day.
Hours 16+: For longer protocols, the benefits deepen. Ketone production increases. Autophagy continues. Inflammatory markers decline further. These require fasting windows beyond daily 16:8 but can be incorporated periodically.
The Research on IF and Insulin Resistance
The clinical evidence has strengthened considerably over the past decade. The consistent finding across multiple study designs is that fasting protocols improve insulin sensitivity beyond what weight loss alone explains — confirming the fasting window itself is driving the benefit.
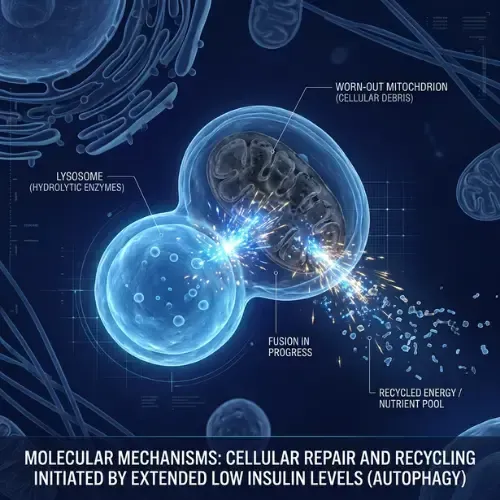
A 2019 review in the New England Journal of Medicine identified four primary pathways: reduction in fasting insulin and insulin resistance; activation of the metabolic switch to fat and ketone oxidation; upregulation of autophagy and cellular stress resistance; and reduction of inflammatory markers including CRP and IL-6. All four are driven by the sustained low-insulin period the fasting window creates — not by caloric restriction per se.
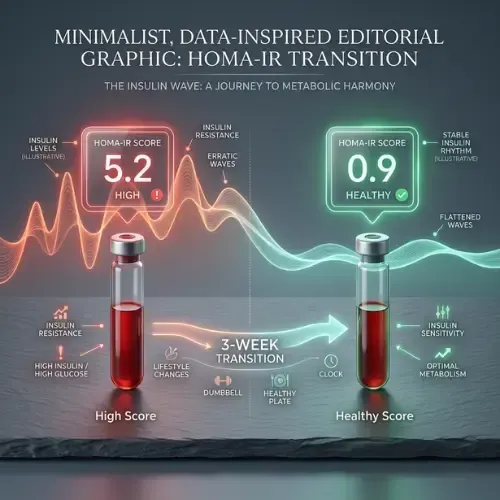
A systematic review and meta-analysis found that intermittent fasting produced significantly greater reductions in fasting insulin and HOMA-IR than continuous calorie restriction, even in studies controlling for total caloric intake, confirming that the timing of food restriction — independent of its caloric effect — has specific beneficial effects on insulin sensitivity. (Harris L et al. — JBI Database of Systematic Reviews, 2018)
What IF Does Beyond Weight Loss:
• Reduces fasting insulin — the primary driver of fat storage and insulin resistance
• Improves HOMA-IR — the most sensitive marker of insulin resistance
• Activates the metabolic switch — from glucose to fat/ketone oxidation
• Upregulates autophagy — cellular repair that declines with metabolic dysfunction
• Reduces visceral fat specifically — TRE research shows preferential visceral fat loss
• Lowers triglycerides — fasting allows VLDL clearance continuous eating prevents
• Reduces CRP and IL-6 — inflammatory markers linked to insulin resistance
• Improves leptin sensitivity — lower fasting insulin reduces hypothalamic inflammation
How to Use Intermittent Fasting for Insulin Resistance — What Actually Works
Start at 12 hours and extend gradually. For someone with insulin resistance, jumping to 16:8 immediately can be difficult — not because it's dangerous but because chronic glucose dependency makes the early fasting period uncomfortable. Finish dinner at 7pm, don't eat until 7am. Within one to two weeks, extend by an hour at a time. Most people reach 14 to 16 hours within a month as metabolic flexibility improves.
What you eat in the window matters enormously. The metabolic benefits of fasting are substantially reduced if the eating window is filled with the refined carbohydrates that drove insulin resistance in the first place. A 16:8 protocol with two high-carbohydrate meals still produces benefits relative to continuous eating — but far less than a 16:8 with meals built around protein, healthy fats, and low-glycemic carbohydrates. The fasting window and the dietary composition are multipliers, not alternatives.
Black coffee and plain tea do not break a metabolic fast. Both are insulin-neutral in normal amounts. Black coffee may actually enhance fasting benefits by mildly stimulating fat oxidation. Adding cream, sugar, or milk does break the fast — the insulin response to dairy protein and carbohydrates is sufficient to suppress the fasting state.
Morning hunger diminishes within two to three weeks. Early morning hunger is primarily a conditioned hormonal response — the trained expectation of breakfast — not genuine metabolic need. As insulin sensitivity improves and fat oxidation establishes, the urgent glucose-crash-driven hunger signal disappears. Hunger in late morning becomes mild and manageable rather than disruptive.
Consistency beats duration. A consistent 14-hour fast every day produces better metabolic outcomes than occasional 20-hour fasts surrounded by unrestricted eating. The adaptations that improve insulin sensitivity — upregulation of fat oxidation enzymes, reduced fasting insulin, improved receptor sensitivity — develop through consistent exposure over weeks, not sporadic long fasts.
What This Means for the MAP30 Challenge
The MAP30 protocol is structured around the fasting principles in this article. The eating window creates a consistent daily low-insulin period that allows the metabolic switch to activate and insulin sensitivity to begin recovering. The dietary framework within that window keeps insulin in a moderate range — preventing the sharp spikes that would undermine the fasting window's benefits.
For people with established insulin resistance, the fasting window is often the most immediately impactful change in the protocol. Not because it produces dramatic weight loss in week one, but because it may be the first time in years that the body's insulin has been consistently low enough for fat burning biology to activate. The changes that follow — declining hunger urgency, improving energy stability, gradual body composition shift — are downstream consequences of that hormonal shift.
The answer to whether intermittent fasting can help with insulin resistance is yes. The evidence is consistent, the mechanism is well-understood, and the practical application is accessible. The question is not whether it works. It is whether you pair it with the dietary changes that allow the fasting window to produce everything it is capable of producing.
This article is part of our Fasting & Metabolic Reset series. Fasting & Metabolic Reset
Latest Articles

Diagnosed With Prediabetes. Now What?
Your fasting glucose came back at 99. Your doctor said everything looks fine. It isn't. Here's what that number actually means.
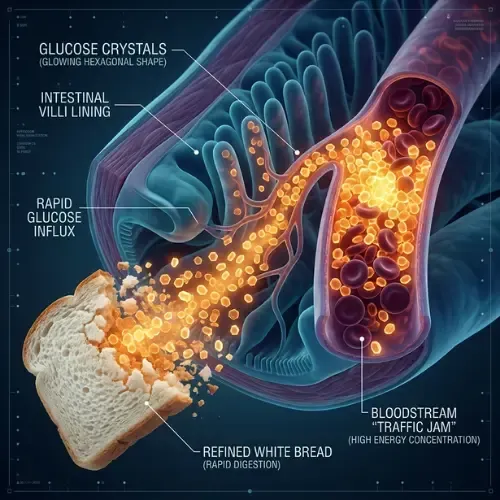
How Insulin Controls Blood Sugar
You eat two slices of white bread with lunch. You didn't add sugar to anything. But in the next 45 minutes, your blood sugar will spike higher.

Water Fasting — What Happens to Your Body
Most people have fasted for 16 hours and called it intermittent fasting. Water fasting is a different thing entirely. Here's what happens.

John Shaw
MAP30 Challenge
John Shaw is a Certified Nutrition Educator and the founder of the MAP30 Challenge. What began as a personal health journey at 294 pounds, and pre-diabetic, evolved into a structured 30-day metabolic reset program grounded in nutritional science. John's mission is simple: give people the biological education that the diet industry never did.
FAQ's
1. Can intermittent fasting help with insulin resistance?
Yes — consistently across multiple randomized controlled trials and systematic reviews. IF improves fasting insulin and HOMA-IR beyond what calorie restriction alone produces, even in studies controlling for total caloric intake. The mechanism is the sustained low-insulin period created by the fasting window — the hours during which insulin falls far enough for insulin sensitivity recovery, fat oxidation, and autophagy to activate.
2. How does intermittent fasting turn on fat burning?
Fat burning activates when insulin falls low enough for hormone-sensitive lipase to release stored fatty acids from adipose tissue. In a continuous eating pattern insulin never reaches this nadir. In a 16:8 protocol, the 16-hour window allows insulin to fall — reaching the threshold around hours 12 to 14 — at which point the metabolic switch activates and fat and ketone oxidation become the primary fuel source.
3. What are the metabolic effects of intermittent fasting beyond weight loss?
Significant reductions in fasting insulin and HOMA-IR; activation of the metabolic switch to fat and ketone oxidation; upregulation of autophagy and cellular repair; preferential visceral fat reduction; lower triglycerides; reduced inflammatory markers including CRP and IL-6; and improved leptin sensitivity. These effects are driven by the fasting window itself — not solely by caloric reduction.
4. How long should you fast to improve insulin resistance?
The threshold for meaningful metabolic benefit appears to be around 12 to 14 hours — the point at which liver glycogen is depleted and the metabolic switch activates. A 16:8 protocol consistently produces significant improvements in insulin sensitivity markers. For people starting from significant insulin resistance, beginning at 12 hours and extending gradually is a practical approach that allows metabolic adaptation without excessive difficulty.
5. Does intermittent fasting 16/8 work for beginners?
Yes — 16:8 is the most studied and accessible IF protocol and the one with the strongest evidence base for insulin resistance specifically. The simplest entry point: stop eating after dinner at 7pm and delay breakfast until 11am. No food is restricted, no calories counted — just the eating window. Most people experience the first significant metabolic improvements within two to three weeks of consistent 16:8.
6. What are the effects of intermittent fasting on metabolism?
IF improves metabolic function through multiple pathways: it lowers fasting insulin allowing fat oxidation and insulin sensitivity to recover; it activates the metabolic switch shifting fuel from glucose to fat and ketones; it upregulates autophagy improving mitochondrial function; and it reduces the visceral fat and chronic inflammation that are primary drivers of metabolic dysfunction. The effects compound over weeks as the body adapts to regular fasting windows.
Sources
Sutton EF et al. — 'Early Time-Restricted Feeding Improves Insulin Sensitivity' (Cell Metabolism, 2018) — https://pubmed.ncbi.nlm.nih.gov/29754952/
de Cabo R, Mattson MP — 'Effects of Intermittent Fasting on Health, Aging, and Disease' (NEJM, 2019) — https://pubmed.ncbi.nlm.nih.gov/31881139/
Harris L et al. — 'Intermittent fasting interventions for treatment of overweight and obesity in adults' (JBI Database, 2018) — https://pubmed.ncbi.nlm.nih.gov/29419624/
Anton SD et al. — 'Flipping the Metabolic Switch' (Obesity, 2018) — https://pubmed.ncbi.nlm.nih.gov/29086496/
Longo VD, Mattson MP — 'Fasting: Molecular Mechanisms and Clinical Applications' (Cell Metabolism, 2014) — https://pubmed.ncbi.nlm.nih.gov/24440038/

Let Me See The Ai Audit Report
I had the MAP30 course material audited and graded by 4 dirrerent Ai models. I was shocked by the grade. See what they had to say about the MAP30 course.
Jaabsha Marketing LLC | All rights reserved 2024 Terms Of Service