17 April, 2026
Edition: Fasting & Metabolic Reset
Vol 1, Edition 32
Time-Restricted Eating vs. Calorie Restriction: Does When You Eat Matter More Than How Much?
Two people eat the same foods and the same number of calories. One eats across a 12-hour window. The other compresses everything into 6 hours. Three months later, their metabolic markers have diverged — not because of what they ate, but because of when.

Published By: MAP30 Challenge | Authored By: John Shaw
Article Directory: https://map30challenge.com/article-directory
The calorie model of weight loss is simple and intuitively appealing: energy in minus energy out equals the change in body weight. Eat less than you burn, lose weight. It is the arithmetic of every diet that has ever been sold, and it is not wrong. Calories matter. But the arithmetic ignores the hormonal environment the timing of those calories creates — and that hormonal environment is where the real metabolic work happens.
Time-restricted eating is the practice of confining food intake to a specific window within the 24-hour day. It does not prescribe what you eat or how much. It defines when. And that single change — compressing the eating window, extending the overnight fast — produces metabolic effects that calorie restriction alone does not consistently replicate. Understanding why requires understanding what happens during the hours you are not eating.
"Time-restricted eating and calorie restriction are not the same intervention. One reduces the quantity of energy input. The other changes the hormonal environment that determines what the body does with that energy — and the difference shows up on a blood test."
What Time-Restricted Eating Actually Is — And What It Isn't
When I started applying time-restricted eating to my own life, I made the same mistake most people make first: I treated the eating window primarily as a calorie control mechanism. Eat in a smaller window, eat less, lose weight. That thinking is not wrong, but it misses the more important mechanism. What I was actually doing — without fully understanding it at the time — was giving my body a longer period each day where insulin was low enough that fat burning could genuinely operate. The window was the intervention. The calorie reduction was secondary.
Time-restricted eating — TRE — is the practice of eating all daily food within a defined window of hours, typically between 6 and 10 hours, and fasting for the remaining 14 to 18 hours. It is sometimes described as a form of intermittent fasting, and the two share mechanisms and benefits. The distinction worth drawing: intermittent fasting is typically framed around the fasting period — the hours of not eating. Time-restricted eating is framed around the eating window — the hours of eating. A 16:8 intermittent fasting protocol and an 8-hour TRE protocol are physiologically identical.
The more important distinction is between time-restricted eating and simple calorie restriction. Calorie restriction reduces total energy intake without necessarily changing when that intake occurs. TRE changes the timing without necessarily restricting the quantity. They are different levers. They produce some overlapping effects and some effects that are genuinely independent — and the research has become increasingly clear about which is which.
The Circadian Biology — Why Your Body Cares What Time You Eat
The human body runs on a 24-hour clock, and every metabolic process follows it. This is not a metaphor. Every organ, every hormone, every enzyme involved in digestion, nutrient storage, and energy burning has a circadian rhythm — a predictable daily pattern of activity and rest that evolved over millions of years of eating during daylight and fasting through the night.
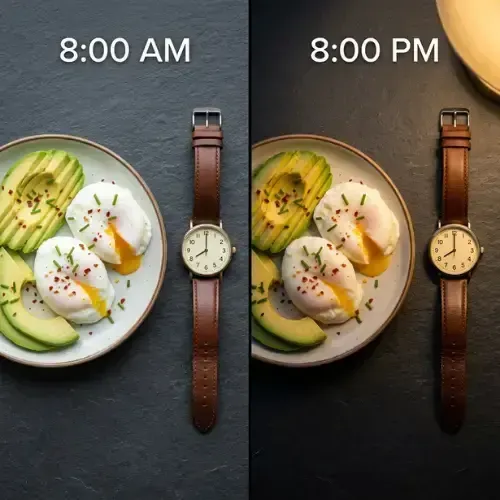
Insulin sensitivity follows this rhythm most consequentially for fat loss. Sensitivity is highest in the morning and declines progressively through the afternoon and evening — meaning the same meal produces a significantly smaller insulin response at 8am than at 8pm. The pancreas secretes less insulin. Blood sugar rises less and falls faster. The body handles carbohydrates more efficiently when the circadian clock says it is the feeding period, and more poorly when it says the feeding period has passed.
The liver tracks this same clock. During the active phase — roughly the first 8 to 10 hours after waking — the liver is primed for glucose uptake, glycogen synthesis, and energy distribution. During the resting phase, the liver shifts toward repair, lipid metabolism, and cleanup processes that require low insulin to function. Eating late in the evening forces the liver to handle nutrient load during the period it is biologically prepared for something else entirely.
Melatonin compounds the problem. As evening progresses, rising melatonin — the sleep hormone — directly suppresses insulin secretion by binding to receptors on pancreatic beta cells. Eating a large meal while melatonin is rising creates two conflicting hormonal signals simultaneously: the body trying to initiate the overnight fasting-and-repair state while insulin is being forced up by a late dinner. The result is impaired glucose clearance, elevated overnight insulin, and a fasting period that never fully lowers before morning eating begins.
A landmark trial found that restricting eating to a 6-hour window in the early part of the day improved insulin sensitivity, blood pressure, and oxidative stress in men with prediabetes even without any weight loss. The metabolic improvements occurred because of timing alone — with no change in caloric intake. (Sutton EF et al. — Cell Metabolism, 2018)
20–50% higher
postprandial glucose and insulin response to identical meals eaten in the evening vs. the morning — the circadian insulin sensitivity gap
Morris CJ et al. — Endocrine Reviews, 2012; Bo S et al. — Nutrients, 2019
What's the Best Fasting Length for Fat Loss — 12h, 16h, or Beyond
Scientists have tested essentially every fasting window combination, and the finding that consistently emerges is that the benefits do not scale linearly — the jump from 12 to 16 hours is far more significant than the jump from 16 to 20. Understanding each window as a decision rather than a point on a scale is what makes this practical.
When I was working to find my own sustainable window, the shift from 12 to 16 hours was the one that changed how I felt day to day — the afternoon energy dips reduced, the sugar cravings softened, and the hunger during the fasting period became predictable rather than urgent. That is the metabolic switch zone doing its work. Here is how each window actually compares:
12 hours — the metabolic baseline — roughly what occurs between finishing dinner at 7pm and eating breakfast at 7am. Research shows 12 hours is sufficient to begin glycogen depletion, allow cortisol to follow its natural overnight arc, and initiate modest fat oxidation. It is the minimum for metabolic benefit and the starting point for anyone new to structured eating windows.
14 to 16 hours — the metabolic switch zone — this is where the meaningful shift occurs. The metabolic switch — the transition from glucose to fat and ketone oxidation — activates most reliably in the 14 to 16 hour range. Glycogen is fully depleted. Growth hormone pulses during sleep are protected. Autophagy upregulates. Fasting insulin reaches its nadir. This is the evidence-supported daily target for most adults pursuing fat loss and metabolic improvement. For the full hour-by-hour physiology of what the body does during a fast, the 24-Hour Fasting article in this library covers that in depth.
18 to 20 hours — extended TRE — compressing the eating window to 4 to 6 hours amplifies the fasting period effects significantly. Ketone production increases. Autophagy deepens. Visceral fat loss in clinical trials is more pronounced. The tradeoff is practicality — a 4-hour eating window requires intentional protein distribution across fewer meals.
36 hours and beyond — extended fasting — a different category of intervention from daily TRE. Multi-day fasts produce substantially deeper autophagy, stem cell activation signals, and glycogen depletion. Covered in the Water Fasting and 24-Hour Fasting articles in this library. Not a daily practice and not required for the MAP30 framework, though periodic extended fasts have documented metabolic benefits.
The practical recommendation: start at 12 hours and add two hours every week until 16 hours feels sustainable. Consistency at 16 hours every day outperforms occasional 20-hour fasts. The window you can maintain is the one that produces results.
TRE vs Calorie Restriction — What the Research Actually Shows
The most important clinical question about time-restricted eating is whether it produces metabolic benefits beyond those attributable to caloric reduction. If TRE only works because people spontaneously eat less within a shorter window, then it is a compliance mechanism for calorie restriction — not a distinct intervention. The controlled research suggests it is genuinely distinct.

The Sutton 2018 Cell Metabolism trial is the most controlled demonstration: metabolic markers improved without weight loss and without caloric restriction. The timing of food intake was the only variable that changed. The metabolic improvements happened because of when the food was eaten, not how much.
A 2020 study found that 14-hour daily TRE in people with metabolic syndrome — without any dietary changes or calorie counting — reduced body weight, decreased visceral fat, lowered blood pressure, improved fasting glucose and insulin, and reduced LDL cholesterol over 12 weeks. Participants simply stopped eating after 10pm and delayed breakfast. Nothing else changed. (Wilkinson MJ et al. — Cell Metabolism, 2020)
Multiple meta-analyses comparing TRE to continuous calorie restriction at matched caloric deficits find that TRE produces equivalent fat loss with greater improvements in fasting insulin and insulin sensitivity — suggesting the hormonal effect of the fasting window operates independently of the caloric effect. The two mechanisms compound when combined, which is exactly why the MAP30 framework pairs dietary composition change with a defined eating window.
12h vs 16h vs 20h: What Changes in Each Fasting Window
12h vs 16h vs 20h: What Changes in Each Fasting Window
Each additional hour of fasting produces meaningfully different metabolic effects — not a linear increase, but distinct biological phases
12 Hours
The metabolic baseline
Insulin
Falling but not yet at nadir. Cells still processing residual signals from last meal.
Liver glycogen
Partially depleted. Gluconeogenesis beginning to supplement.
Fat burning
Beginning to activate. Not yet primary fuel source.
Autophagy
Basal level. Meaningful upregulation has not yet begun.
Circadian alignment
Standard overnight fast — what human biology was designed for.
Best for
Starting point. Better than constant eating. Foundation to build from.
16 Hours
The evidence-supported sweet spot
Insulin
At genuine nadir. mTOR inhibited. Fat cells unlocked for mobilization.
Liver glycogen
Largely depleted. Metabolic switch activates — fat and ketones become primary fuel.
Fat burning
Well established. Fatty acids mobilized from adipose. Ketone production begins.
Autophagy
Meaningfully upregulated. Cellular cleanup and mitophagy active.
Growth hormone
Rising. Supports lean mass preservation and overnight fat mobilization.
Best for
Daily fat loss, insulin resistance reversal, metabolic health maintenance.
20 Hours
Extended TRE — deeper adaptation
Insulin
Deeply suppressed. Maximum fat cell unlocking. Strongest metabolic flexibility signal.
Liver glycogen
Fully depleted. Liver running primarily on fat and ketones.
Fat burning
Deep fat oxidation. Ketone levels measurably elevated. Brain running on ketones.
Autophagy
Robustly activated. Deeper cellular maintenance than 16h produces.
Protein timing
Requires deliberate planning — adequate protein across 4-hour window needs intention.
Best for
People with good metabolic flexibility who want to deepen the adaptation.
Is Intermittent Fasting Destroying Your Hormones — Or Is That the Wrong Question
The claim that intermittent fasting destroys hormones is one of the most common objections I hear — particularly from women and from anyone over 40. I want to be clear: the concern is based on real biology that has been significantly misapplied. The full picture depends almost entirely on which hormones, which fasting protocol, and crucially, what time of day the eating window falls.
The hormonal concern typically centers on cortisol. Extended fasting does raise cortisol — cortisol is one of the mechanisms the body uses to release glucose when blood sugar falls. For daily TRE in the 14 to 16 hour range, this cortisol response is modest and transient. For multi-day fasting or very compressed windows in already-stressed individuals, the cortisol response becomes more significant and warrants attention. The protocol matters enormously, and daily TRE is not the same biological stimulus as a 72-hour fast.
What early TRE consistently does to hormones is improve them. Aligning eating with the first 8 to 10 hours of the day and fasting through the evening and overnight produces a measurably different hormonal outcome than the common pattern of eating from noon through 10pm. The research on early versus late TRE makes the distinction clear: earlier windows produce better insulin sensitivity, better cortisol rhythm, and better growth hormone pulses — because they align with the circadian biology rather than working against it.
For practical daily TRE, the guidelines that produce the best hormonal outcomes:
Choose a consistent eating window of 6 to 8 hours — consistency matters as much as length — the circadian system responds to predictable patterns, and an irregular window undermines the adaptation
Avoid eating in the 2 to 3 hours before sleep — this is where melatonin-insulin conflict does the most hormonal damage — late eating elevates overnight insulin and suppresses the growth hormone pulse that should occur during early sleep
Front-load calories when possible — eating more in the first half of the eating window and less in the second half aligns intake with peak circadian insulin sensitivity and produces better glucose and insulin responses
Start gradually — moving from 12 to 14 to 16 hours over several weeks allows ghrelin and hunger hormones to adapt without triggering a stress response — the adaptation is real and takes two to three weeks
Prioritize protein within the window — adequate protein within a compressed eating window preserves lean mass and prevents the muscle catabolism that would genuinely raise cortisol and worsen the hormonal picture
When intermittent fasting is done with the circadian rhythm rather than against it, it consistently improves the hormonal markers that matter most: fasting insulin falls, growth hormone pulses deepen, leptin sensitivity improves, and the cortisol diurnal rhythm normalizes. The fasting that damages hormones is underfueled, poorly timed, or applied to a body already under significant metabolic stress. Structured daily TRE is not that.
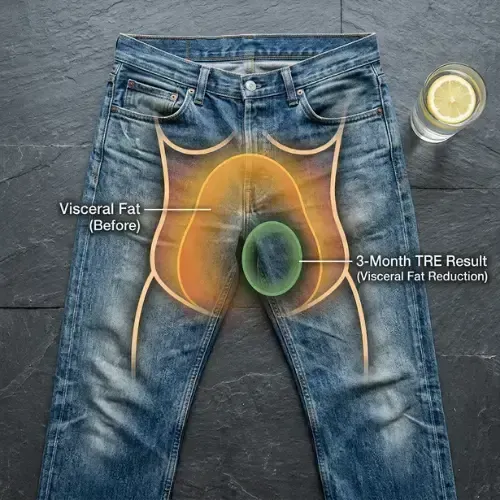
Time-Restricted Eating and Visceral Fat
One of the most clinically significant findings in the TRE literature is that time-restricted eating appears to preferentially reduce visceral fat — the metabolically active fat that accumulates around the liver, pancreas, and intestines and drives insulin resistance, inflammation, and cardiovascular risk — beyond what total weight loss would predict.
The mechanism is consistent with the circadian biology. By extending the overnight fasting period and aligning eating with the circadian window of peak insulin sensitivity, TRE creates conditions where the liver and visceral adipose tissue are clearing stored fat during the fasting period rather than cycling continuously between storage and partial mobilization. Visceral fat is particularly insulin-sensitive — it responds more dramatically to insulin reduction than subcutaneous fat. The extended insulin-low state that daily TRE produces preferentially targets the fat that poses the greatest metabolic risk.
As covered in the Visceral Fat article in this library, visceral fat is the primary driver of the inflammatory and insulin-disrupting consequences of metabolic dysfunction. Interventions that specifically reduce visceral fat produce disproportionate metabolic benefits relative to the scale weight lost. The research consistently finding visceral fat reduction in TRE trials, beyond what total weight loss would predict, is the clearest evidence that the timing mechanism is doing independent metabolic work. The combination of dietary quality plus a defined eating window is what the MAP30 framework is built around — and this is precisely why.
This article is part of our Fasting & Metabolic Reset series. Fasting & Metabolic Reset
Latest Articles
How a Low-Carb Diet Works
Keto. Low-carb. Carbohydrate restriction. Metabolic eating. The names change. The biology doesn't. When you stop sending your body the foods that spike insulin.

Fat for Heart Disease
In 1967, the New England Journal of Medicine published a landmark review concluding that fat and cholesterol caused heart disease — and that sugar was not the problem.

Why Are Seed Oils Bad
Seed oils are in almost everything processed food contains. They are marketed as heart-healthy vegetable oils. They are a product of industrial chemistry.

John Shaw
MAP30 Challenge
John Shaw is a Certified Nutrition Educator and the founder of the MAP30 Challenge. What began as a personal health journey at 294 pounds, and pre-diabetic, evolved into a structured 30-day metabolic reset program grounded in nutritional science. John's mission is simple: give people the biological education that the diet industry never did.
FAQ's
1. What is the best fasting length for fat loss — 12h, 16h, or 36h?
14 to 16 hours is the evidence-supported daily target — the window where the metabolic switch activates reliably for most people. Glycogen is fully depleted, fat and ketone oxidation establish, growth hormone fires, and autophagy upregulates. 12 hours is the metabolic baseline. 18 to 20 hours deepens the adaptation. 36 hours and beyond is a different category of protocol with different biology — covered in the 24-Hour Fasting and Water Fasting articles in this library. For daily sustainable practice, consistent 16 hours outperforms less frequent longer fasts.
2. Is time-restricted eating the same as calorie restriction?
No — and the distinction matters. Calorie restriction reduces total energy intake without necessarily changing when that intake occurs. Time-restricted eating changes the timing without necessarily restricting the quantity. Clinical trials including the Sutton 2018 Cell Metabolism study have demonstrated TRE produces improvements in insulin sensitivity, blood pressure, and oxidative stress even without weight loss or caloric reduction — driven by the circadian biology of nutrient timing rather than energy quantity.
3. Does it matter what time of day the eating window falls?
Yes significantly. Earlier windows — eating in the first 8 to 10 hours after waking — align with peak circadian insulin sensitivity and produce the greatest metabolic benefits per unit of window length. Late windows eating from noon through 10pm capture some fasting benefits while eating into the period of declining insulin sensitivity and rising melatonin. For most people, any consistent window is better than no window. But earlier is consistently better than later when the research directly compares them.
4. What is circadian fasting?
Circadian fasting refers to aligning the eating window with the body's circadian metabolic rhythm — specifically, eating during the hours of peak insulin sensitivity (roughly the first 8 to 10 hours after waking) and fasting during the evening and overnight when metabolic efficiency declines and repair processes require low insulin to operate. It is time-restricted eating with explicit attention to the circadian timing of the window, not just its length.
5. Is intermittent fasting bad for hormones?
Daily TRE in the 14 to 16 hour range consistently improves the hormonal markers that matter most for metabolic health — fasting insulin, growth hormone, leptin sensitivity, and cortisol diurnal rhythm — when the eating window is adequately fueled and reasonably timed. The concern about hormonal damage applies more specifically to very compressed windows in already-stressed individuals, or to multi-day fasting protocols, not to structured daily TRE.
6. How does time-restricted eating affect visceral fat?
TRE appears to preferentially reduce visceral fat beyond what total weight loss would predict. The mechanism involves the extended insulin-low state during the fasting period, which gives visceral adipose tissue the hormonal conditions to release stored fat. Visceral fat is highly insulin-sensitive and responds disproportionately to the insulin reduction that daily TRE produces.
Sources
Sutton EF et al. — 'Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes' (Cell Metabolism, 2018) — https://pubmed.ncbi.nlm.nih.gov/29754952/
Wilkinson MJ et al. — 'Ten-Hour Time-Restricted Eating Reduces Weight, Blood Pressure, and Atherogenic Lipids in Patients with Metabolic Syndrome' (Cell Metabolism, 2020) — https://pubmed.ncbi.nlm.nih.gov/31813881/
Morris CJ et al. — 'Circadian system, sleep and endocrinology' (Molecular and Cellular Endocrinology, 2012) — https://pubmed.ncbi.nlm.nih.gov/22484406/
Lowe DA et al. — 'Effects of Time-Restricted Eating on Weight Loss and Other Metabolic Parameters in Women and Men With Overweight and Obesity' (JAMA Internal Medicine, 2020) — https://pubmed.ncbi.nlm.nih.gov/32986097/
Regmi P, Heilbronn LK — 'Time-Restricted Eating: Benefits, Mechanisms, and Challenges in Translation' (iScience, 2020) — https://pubmed.ncbi.nlm.nih.gov/32526749/

Let Me See The Ai Audit Report
I had the MAP30 course material audited and graded by 4 dirrerent Ai models. I was shocked by the grade. See what they had to say about the MAP30 course.
Jaabsha Marketing LLC | All rights reserved 2024 Terms Of Service