13 April, 2026
Edition: Insulin & Blood Sugar
Vol 2, Edition 6
How a Low-Carb Diet Works — And Why It Doesn't Matter What You Call It
Keto. Low-carb. Carbohydrate restriction. Metabolic eating. The names change. The biology doesn't. When you stop sending your body the foods that spike insulin, something predictable happens — and it has nothing to do with which dietary tribe you belong to.

Published By: MAP30 Challenge | Authored By: John Shaw
Article Directory: https://map30challenge.com/article-directory
I want to be honest with you about something before we get into the biology. I don't care what you call this. In the MAP30 program I tell people the same thing every time: it doesn't matter if you call it keto, low-carb, metabolic eating, or nothing at all. As long as you're eating foods that don't spike insulin and staying under 50 grams of carbs a day, you are doing the thing. I'm not interested in technical terms. I'm interested in helping people change their lives. The label is irrelevant. The biology is not.
Strip away the terminology and what remains is one foundational principle: when you reduce the foods that spike insulin, your body's hormonal environment shifts. Insulin falls. Fat burning activates. Hunger stabilizes. The metabolic dysfunction that had been building quietly for years begins to reverse. The food determines the signal. The name you give the diet is irrelevant.
MAP30 does not require you to identify as keto or low-carb or anything else. It asks you to understand the mechanism — why certain foods produce the hormonal environment that stores fat and others produce the environment that releases it — and to make choices based on that understanding rather than on a dietary label. This article explains the mechanism. What you call it afterward is entirely up to you.
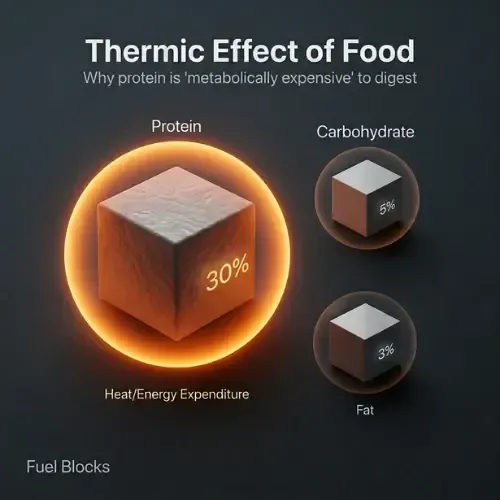
"Protein is not a supplement to a fat loss strategy. For most people, it is the fat loss strategy — and every other dietary change they are making is working against them because they are not eating enough of it."
What a Low-Carb Diet Actually Is — Cutting Through the Confusion
A low-carbohydrate diet is any dietary pattern that reduces carbohydrate intake below the level that maintains chronic insulin elevation. There is no single threshold — the effective range varies by individual, by the degree of existing insulin resistance, and by what else is in the diet. But the general territory is well-defined by research:
Very low carbohydrate / ketogenic: under 20 to 50 grams of total carbohydrates per day. Produces consistent nutritional ketosis — the liver is producing ketones from fat as the primary fuel source. Maximum insulin reduction.
Low carbohydrate: 50 to 130 grams per day. Produces significant insulin reduction without necessarily achieving full ketosis. Effective for insulin resistance reversal and fat loss in most people.
Moderate carbohydrate restriction: 130 to 200 grams per day, with emphasis on low-glycemic sources. Produces meaningful improvements in metabolic markers compared to the standard Western diet while being more flexible for many people.
The MAP30 target of staying under 50 grams of carbohydrates per day lands in the very-low-carbohydrate range — the zone where insulin reduction is most reliable and where the metabolic switch to fat burning activates most consistently. But the more important principle is not the number. It is the food quality. Fifty grams of carbohydrates from vegetables, berries, and whole foods produces a very different metabolic response than 50 grams from bread and processed snacks. The source matters alongside the quantity.
The Insulin Mechanism — Why Carbohydrate Reduction Works
Understanding that insulin was the primary hormonal driver of fat storage — not calories, not dietary fat, not willpower — was the moment everything changed for me. Once I understood that, the question stopped being "how do I eat less" and became "how do I keep insulin lower for longer." The answer was carbohydrate reduction. And everything that followed confirmed it.
Every other section of this article rests on one foundational fact: insulin is the primary hormonal signal that determines whether your body is storing fat or burning it. When insulin is elevated, fat cells are biochemically locked — hormone-sensitive lipase, the enzyme that releases stored fat for fuel, is suppressed. When insulin falls, fat cells unlock. Stored energy can be released and burned. You cannot be in fat-burning mode and have elevated insulin simultaneously. These states are mutually exclusive.

Carbohydrates — specifically refined carbohydrates and added sugars — are the primary driver of insulin elevation. As covered in the Blood Sugar and Insulin article in this library, refined carbohydrates break down rapidly into glucose, enter the bloodstream quickly, and trigger large, fast insulin responses. When this pattern repeats three or more times a day, insulin is chronically elevated. Fat cells stay locked. Fat burning is suppressed continuously. The metabolic dysfunction accumulates.
Reducing carbohydrate intake interrupts this cycle at the source. Lower carbohydrate intake means smaller, less frequent glucose spikes. Smaller spikes mean lower insulin responses. Lower insulin means fat cells unlock. Fat oxidation activates. The hormonal environment that drives fat storage begins to reverse — not because calories were restricted, though that often follows naturally, but because the primary hormonal driver of fat storage was removed.
A systematic review and meta-analysis of randomized controlled trials found that low-carbohydrate diets produced significantly greater reductions in fasting insulin, triglycerides, and blood pressure, and greater improvements in HDL cholesterol — independent of differences in weight loss between groups. The metabolic improvements occurred beyond what caloric restriction alone could explain. (Mansoor N et al. — British Journal of Nutrition, 2016)
Low-Carb vs Keto — Is There a Difference That Matters
Technically yes. Practically, for most people pursuing metabolic health rather than performance optimization, the distinction matters less than either camp typically suggests.
Strict ketogenic diets — under 20 to 50 grams of carbohydrates per day — reliably produce nutritional ketosis: blood ketone levels above 0.5 mmol/L, indicating the liver is producing ketones as the primary alternative fuel. The additional metabolic benefits of ketosis beyond low-carb include enhanced fat oxidation, potential cognitive benefits from ketone availability, and accelerated visceral fat loss. For people with significant insulin resistance, type 2 diabetes, or neurological conditions, the strict ketogenic range may produce better outcomes.
The low-carbohydrate range — 50 to 130 grams per day — produces most of the same insulin-lowering and fat-burning benefits without requiring the strict macro tracking and food restriction of full ketogenic eating. It is more flexible, more sustainable for most people over the long term, and still produces consistent improvements in fasting insulin, HOMA-IR, triglycerides, and body composition.
Low-Carb vs Keto — How They Compare
| What Changes | Low-Carb (50–130g) | Ketogenic (<50g) |
|---|---|---|
| Insulin reduction | Significant | Maximum |
| Ketone production | Minimal to none | Consistent nutritional ketosis |
| Fat loss | Consistent | Faster initial results |
| Flexibility | High — easier to sustain long term | Low — requires strict tracking |
| Best for | Most people starting out | Significant insulin resistance or T2D |
The honest answer for most people: start with the low-carbohydrate range, see how your body responds, and adjust from there. If you are not seeing the metabolic improvements you expect, tighten toward the ketogenic range. If the low-carbohydrate range is producing the results you are looking for, there is no metabolic reason to go lower. The goal is not adherence to a specific dietary identity. The goal is the hormonal environment the diet produces.
Under 50g carbs per day
is the MAP30 target — the zone where insulin reduction is most reliable and the metabolic switch to fat burning activates most consistently
Anton SD et al. — Flipping the Metabolic Switch, Obesity, 2018
Is a Low-Carb Diet Destroying Your Heart — Or Is That the Wrong Question
The most persistent criticism of low-carbohydrate eating is cardiovascular — the idea that replacing carbohydrates with fat raises cholesterol and drives heart disease. It is the concern that keeps more people from trying this approach than any other single objection, and it deserves a direct, honest answer rather than a defensive one.
The fear has a specific origin. It traces back to Ancel Keys' Seven Countries Study from the 1950s and 60s, which established the hypothesis that dietary fat — particularly saturated fat — raises LDL cholesterol and causes cardiovascular disease. That hypothesis shaped decades of dietary guidelines and produced the low-fat era. What it did not produce was a reduction in cardiovascular disease, obesity, or metabolic syndrome. All three accelerated during the years when fat was being systematically removed from the food supply and replaced with refined carbohydrates. The hypothesis made a prediction. The data went the other direction.
The actual lipid picture on low-carbohydrate eating tells a more complete story. Yes, LDL cholesterol may rise modestly in some people — and this is the data point that drives the concern. But LDL is not a single uniform measure. The particles matter. Large, buoyant LDL particles carry a dramatically lower cardiovascular risk than small, dense LDL particles. Low-carbohydrate eating consistently shifts the LDL particle pattern toward the less atherogenic type. Meanwhile, triglycerides — one of the most reliable predictors of cardiovascular risk — fall reliably and significantly. HDL rises. And the triglyceride-to-HDL ratio, which research consistently identifies as more predictive of cardiovascular events than LDL alone, improves across the board.
What this means in simple terms: the number your doctor shows you on a standard lipid panel — total LDL — is telling you one part of the story while hiding the more important part. Think of it like judging traffic danger by counting the number of vehicles on the road without distinguishing between school buses and motorcycles. The vehicle count goes up, but the risk profile depends entirely on what kind of vehicles they are. Low-carbohydrate eating may add more school buses to the road while removing the motorcycles. The count looks worse. The road is actually safer.

What actually drives cardiovascular risk is insulin resistance and metabolic syndrome — elevated triglycerides, low HDL, visceral fat, hypertension, and impaired glucose regulation, all operating together. These are the downstream consequences of chronic carbohydrate overload and the insulin elevation it produces. A dietary approach that reduces all five of those markers simultaneously is not increasing cardiovascular risk. It is addressing the metabolic conditions that create it.
What to Eat on a Low-Carb Diet — The Practical Framework
The foods that support the MAP30 low-carbohydrate framework share one characteristic: they do not produce significant insulin spikes. Everything else is secondary. The specific foods you choose within this framework are a matter of preference, practicality, and what you actually enjoy eating.
The transition to a low-carbohydrate eating pattern is not about eliminating pleasure from food. It is about redirecting it. I went through this transition myself — and I'll be honest, the first week was not easy. The body has been running on glucose for years. The cravings are real. The fatigue is real. What I didn't expect was how quickly it shifted. By week two, the hunger that had been driving my eating decisions had quieted down in a way I hadn't experienced before. The foods on the right side of the comparison card started to feel genuinely satisfying — not because I was forcing myself, but because the hormonal environment driving the cravings had changed.
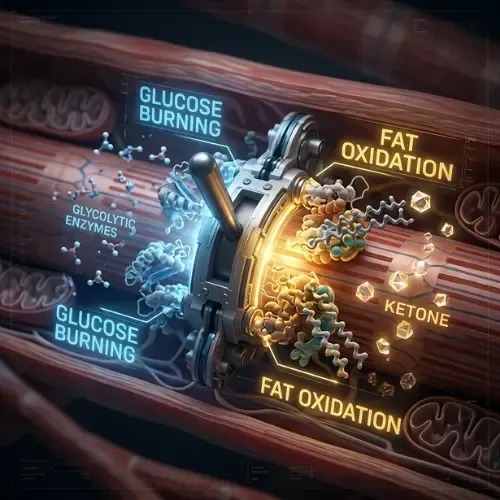
The transition period — the first one to two weeks — is often the hardest. The body is adapting from glucose dependence to fat burning, the enzymatic machinery for fat oxidation is upregulating, and the brain is adjusting to a new fuel environment. This period can produce fatigue, brain fog, and irritability — sometimes called keto flu. It is temporary. It is a sign that the metabolic switch is flipping. It passes. The metabolic health that follows it does not.
This article is part of our Insulin & Blood Sugar series
Latest Articles
Intermittent Fasting Help With Insulin Resistance
Intermittent fasting is the most talked-about dietary intervention of the past decade. But most of the conversation focuses on weight loss.
Protein For Weight Loss
Of the three macronutrients, protein is the one that most directly supports fat loss, preserves lean mass, and keeps hunger manageable. But most people eat far too little of it.

Is Sleep Slowing Your Metabolism
You're doing everything right — eating well, staying active, managing stress as best you can. And yet the scale won't move, your energy is flat.

John Shaw
MAP30 Challenge
John Shaw is a Certified Nutrition Educator and the founder of the MAP30 Challenge. What began as a personal health journey at 294 pounds, and pre-diabetic, evolved into a structured 30-day metabolic reset program grounded in nutritional science. John's mission is simple: give people the biological education that the diet industry never did.
FAQ's
1. How does a low-carb diet work?
A low-carbohydrate diet works by reducing the primary dietary driver of chronic insulin elevation — refined carbohydrates and added sugars. Lower carbohydrate intake means smaller, less frequent glucose spikes. Smaller spikes mean lower insulin responses. Lower insulin means fat cells unlock — hormone-sensitive lipase is freed to release stored fatty acids for fuel. Fat burning activates. The hormonal environment that drives fat storage reverses. The mechanism is hormonal, not caloric.
2. Is a low-carb diet good or bad?
The research on low-carbohydrate eating consistently shows improvements in the metabolic markers that matter most: reduced fasting insulin, lower HOMA-IR, decreased triglycerides, higher HDL, reduced visceral fat, improved blood pressure, and better blood glucose control. For people with insulin resistance, prediabetes, type 2 diabetes, or metabolic syndrome — which describes the majority of Western adults — a low-carbohydrate dietary pattern addresses the underlying metabolic dysfunction more directly than any other dietary approach.
3. What is the difference between keto and low-carb?
Ketogenic eating restricts carbohydrates to under 20 to 50 grams per day, consistently producing nutritional ketosis — liver-derived ketone production above 0.5 mmol/L. Low-carbohydrate eating sits in the 50 to 130 gram range — producing significant insulin reduction and metabolic improvement without necessarily achieving full ketosis. Both produce most of the same benefits. Strict keto may produce faster initial results for people with significant insulin resistance. The low-carbohydrate range is more flexible and sustainable for most people long-term.
4. How to switch to a low-carb diet?
The most effective transition: remove refined carbohydrates and added sugars first — bread, pasta, white rice, cereals, sweetened drinks, processed snacks. Replace them with protein-rich whole foods, healthy fats, and low-glycemic vegetables. The first one to two weeks may involve fatigue and brain fog as the metabolic switch occurs. This is temporary. Extending the overnight fasting window to 12 to 14 hours during the transition accelerates the adaptation. Within two to three weeks, hunger stabilizes, cravings for refined carbohydrates weaken, and energy becomes more consistent.
5. Is a low-carb diet good for weight loss?
Yes — and the mechanism is hormonal, not caloric. Low-carbohydrate eating reduces fasting insulin, unlocks fat cells for fat oxidation, improves satiety signaling through protein emphasis and stable blood sugar, and reduces the hunger and cravings that make dietary adherence difficult. Multiple systematic reviews and meta-analyses show low-carbohydrate diets produce equivalent or greater fat loss than low-fat diets at similar caloric intake, with significantly greater improvements in metabolic markers.
6. What is a low-carb low-sugar diet for fat loss?
A low-carb low-sugar approach removes the two primary drivers of chronic insulin elevation — refined carbohydrates and added sugars — and replaces them with whole food proteins, healthy fats, and low-glycemic vegetables. The MAP30 target of under 50 grams of carbohydrates per day, emphasizing carbohydrates from non-starchy vegetables and whole food sources rather than grains and processed foods, is the practical expression of this approach. It is not a named diet. It is a description of the foods that produce the hormonal environment required for fat loss.
Sources
Mansoor N et al. — 'Effects of low-carbohydrate diets versus low-fat diets on body weight and cardiovascular risk factors' (Br J Nutr, 2016) — https://pubmed.ncbi.nlm.nih.gov/26768850/
Ludwig DS, Ebbeling CB — 'The carbohydrate-insulin model of obesity' (JAMA Internal Medicine, 2018) — https://pubmed.ncbi.nlm.nih.gov/29971406/
Anton SD et al. — 'Flipping the Metabolic Switch' (Obesity, 2018) — https://pubmed.ncbi.nlm.nih.gov/29086496/
Westman EC et al. — 'Low-carbohydrate nutrition and metabolism' (Am J Clin Nutr, 2007) — https://pubmed.ncbi.nlm.nih.gov/17684196/
Volek JS, Phinney SD — 'The Art and Science of Low Carbohydrate Performance' (Beyond Obesity, 2012)

Let Me See The Ai Audit Report
I had the MAP30 course material audited and graded by 4 dirrerent Ai models. I was shocked by the grade. See what they had to say about the MAP30 course.
Jaabsha Marketing LLC | All rights reserved 2024 Terms Of Service